

The ClearSight System for Postoperative Arterial Blood Pressure Monitoring After Carotid Endarterectomy: A Validation Study
- PMID: 34505631
- PMCID: PMC8807161
- DOI: 10.1093/ajh/hpab140
The ClearSight System for Postoperative Arterial Blood Pressure Monitoring After Carotid Endarterectomy: A Validation Study
Abstract
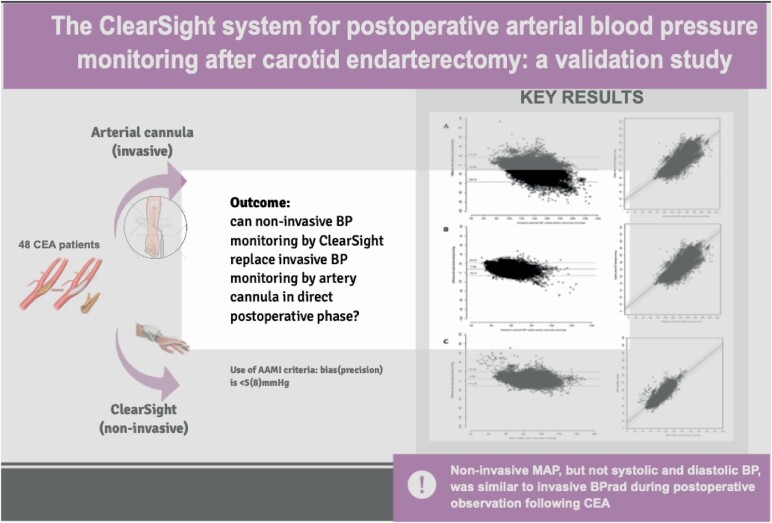
Background: The majority of postoperative events in patients undergoing carotid endarterectomy (CEA) are of hemodynamic origin, requiring preventive strict postoperative arterial blood pressure (BP) control. This study aimed to assess whether BP monitoring with noninvasive beat-to-beat ClearSight finger BP (BPCS) can replace invasive beat-to-beat radial artery BP (BPRAD) in the postoperative phase.
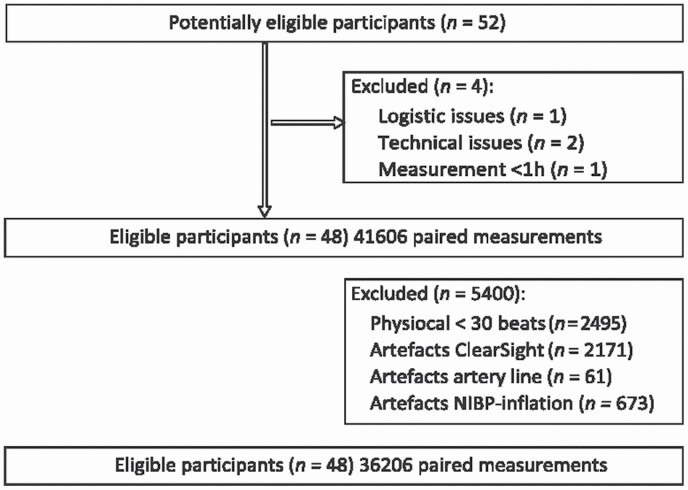
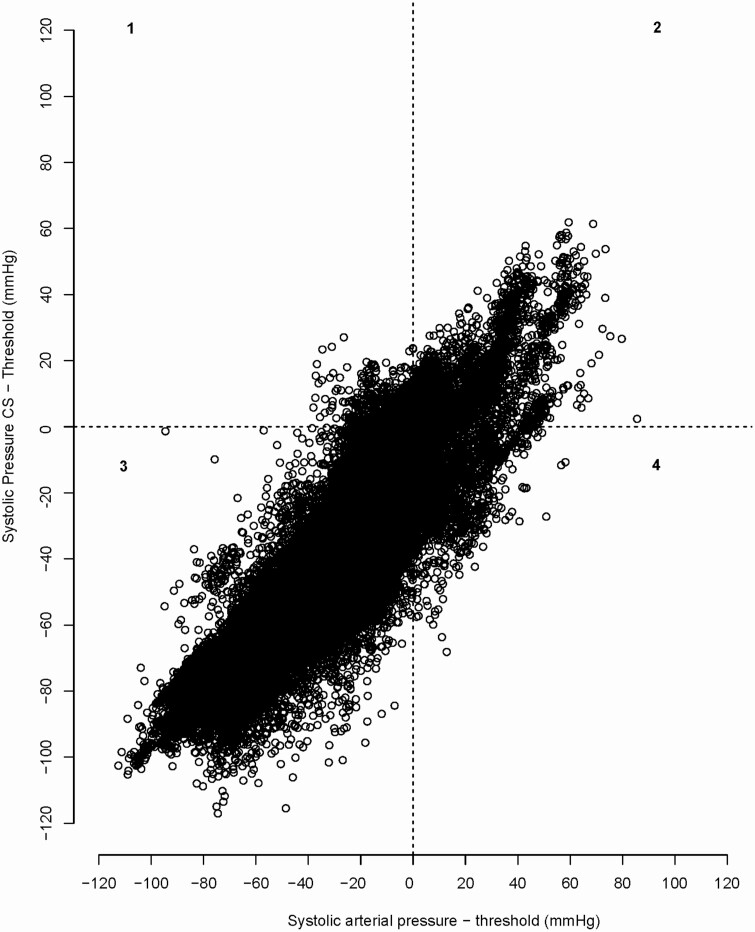
Methods: This study was a single-center clinical validation study using a prespecified study protocol. In 48 patients with symptomatic carotid artery stenosis, BPCS and BPRAD were monitored ipsilateral in a simultaneous manner during a 6-hour period on the recovery unit following CEA. Primary endpoints were accuracy and precision of BP derived by ClearSight (Edward Lifesciences, Irvine, CA) vs. the reference standard (Arbocath 20 G, Hospira, Lake Forest, IL) to investigate if BPCS is a reliable noninvasive alternative for BP monitoring postoperatively in CEA patients. Validation was guided by the standard set by the Association for Advancement of Medical Instrumentation (AAMI), considering a BP-monitor adequate when bias (precision) is <5 (8) mm Hg. Secondary endpoint was percentage under- and overtreatment, defined as exceedance of individual postoperative systolic BP threshold by BPRAD or BPCS in contrast to BPCS or BPRAD, respectively.
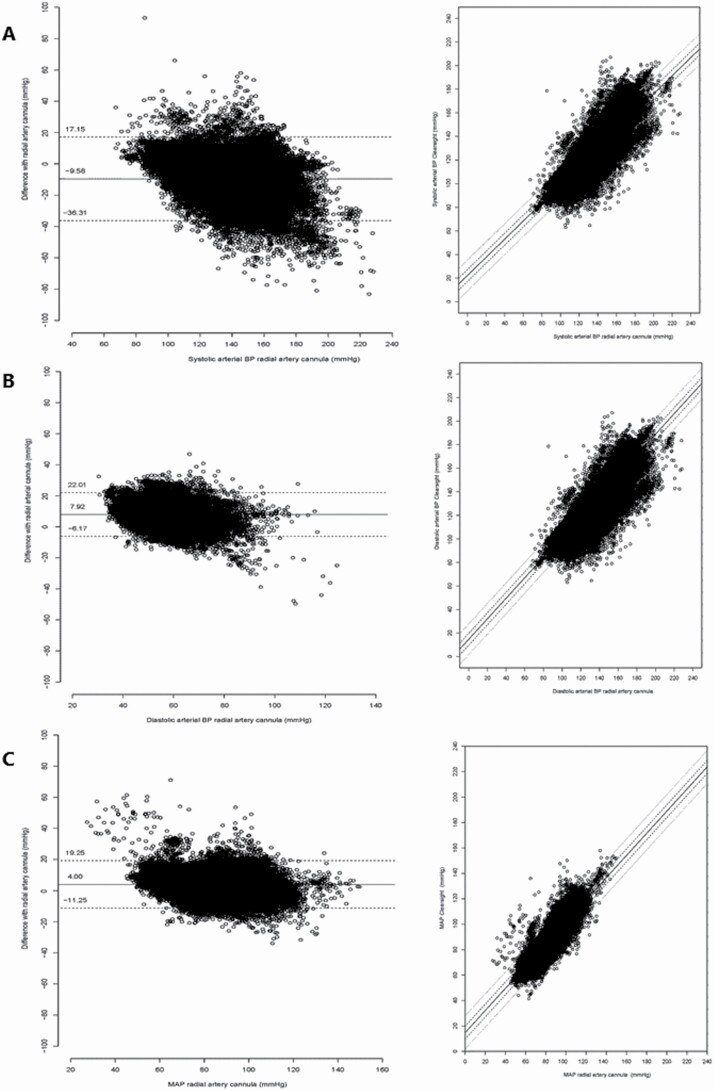
Results: The bias (precision) of BPCS compared to BPRAD was -10 (13.6), 8 (7.2) and 4 (7.8) mm Hg for systolic, diastolic and mean arterial pressure (MAP), respectively. Based on BPCS, undertreatment was 5.6% and overtreatment was 2.4%; however, percentages of undertreatment quadrupled for lower systolic BP thresholds.
Conclusions: Noninvasive MAP, but not systolic and diastolic BP, was similar to invasive BPRAD during postoperative observation following CEA, based on AAMI criteria. However, as systolic BP is currently leading in postoperative monitoring to adjust BP therapy on, BPCS is not a reliable alternative for BPRAD.
Keywords: ClearSight; arterial pressure; blood pressure; carotid endarterectomy; hypertension; noninvasive continuous arterial pressure measurement; postoperative monitoring.
© The Author(s) 2021. Published by Oxford University Press on behalf of American Journal of Hypertension, Ltd.
Figures
References
-
- Ederle J, Dobson J, Featherstone RL, Bonati LH, van der Worp HB, de Borst GJ, Lo TH, Gaines P, Dorman PJ, MacDonald S, Lyrer PA, Hendriks JM, McCollum C, Nederkoorn PJ, Brown MM. Carotid artery stenting compared with endarterectomy in patients with symptomatic carotid stenosis (International Carotid Stenting Study): an interim analysis of a randomised controlled trial. Lancet 2010; 375:985–997. - PMC - PubMed
-
- de Borst GJ, Naylor AR. In the end, it all comes down to the beginning! Eur J Vasc Endovasc Surg 2015; 50:271–272. - PubMed
-
- Naylor AR, Ricco JB, de Borst GJ, Debus S, de Haro J, Halliday A, Hamilton G, Kakisis J, Kakkos S, Lepidi S, Markus HS, McCabe DJ, Roy J, Sillesen H, van den Berg JC, Vermassen F, Kolh P, Chakfe N, Hinchliffe RJ, Koncar I, Lindholt JS, Vega de Ceniga M, Verzini F, Archie J, Bellmunt S, Chaudhuri A, Koelemay M, Lindahl AK, Padberg F, Venermo M, ESVS Guidelines Committee, ESVS Guideline Reviewers. Management of atherosclerotic carotid and vertebral artery disease: 2017 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018; 55:1–79. - PubMed
-
- Huibers A, Calvet D, Kennedy F, Czuriga-Kovács KR, Featherstone RL, Moll FL, Brown MM, Richards T, de Borst GJ. Mechanism of procedural stroke following carotid endarterectomy or carotid artery stenting within the International Carotid Stenting Study (ICSS) randomised trial. Eur J Vasc Endovasc Surg 2015; 50:281–288. - PMC - PubMed
-
- de Borst GJ, Moll FL, van de Pavoordt HD, Mauser HW, Kelder JC, Ackerstaf RG. Stroke from carotid endarterectomy: when and how to reduce perioperative stroke rate? Eur J Vasc Endovasc Surg 2001; 21:484–489. - PubMed
