

Mutation location and IKs regulation in the arrhythmic risk of long QT syndrome type 1: the importance of the KCNQ1 S6 region
- PMID: 34505893
- PMCID: PMC8851466
- DOI: 10.1093/eurheartj/ehab582
Mutation location and IKs regulation in the arrhythmic risk of long QT syndrome type 1: the importance of the KCNQ1 S6 region
Abstract
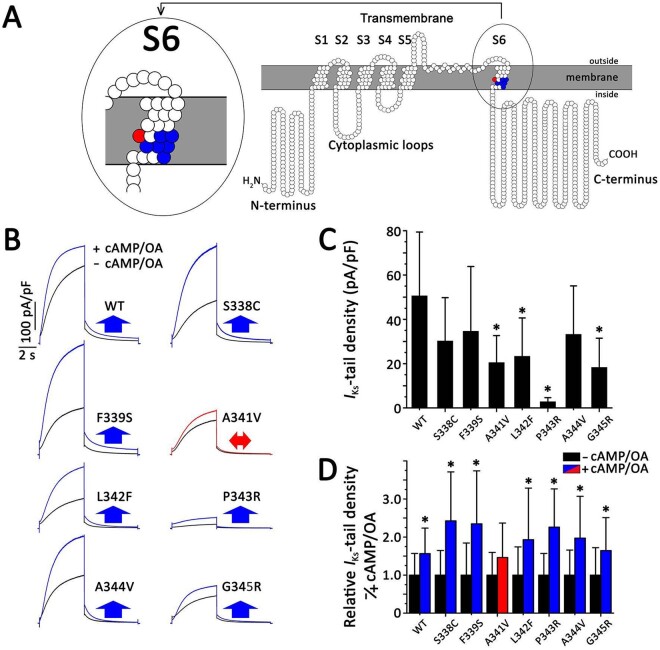
Aims: Mutation type, location, dominant-negative IKs reduction, and possibly loss of cyclic adenosine monophosphate (cAMP)-dependent IKs stimulation via protein kinase A (PKA) influence the clinical severity of long QT syndrome type 1 (LQT1). Given the malignancy of KCNQ1-p.A341V, we assessed whether mutations neighbouring p.A341V in the S6 channel segment could also increase arrhythmic risk.
Methods and results: Clinical and genetic data were obtained from 1316 LQT1 patients [450 families, 166 unique KCNQ1 mutations, including 277 p.A341V-positive subjects, 139 patients with p.A341-neighbouring mutations (91 missense, 48 non-missense), and 900 other LQT1 subjects]. A first cardiac event represented the primary endpoint. S6 segment missense variant characteristics, particularly cAMP stimulation responses, were analysed by cellular electrophysiology. p.A341-neighbouring mutation carriers had a QTc shorter than p.A341V carriers (477 ± 33 vs. 490 ± 44 ms) but longer than the remaining LQT1 patient population (467 ± 41 ms) (P < 0.05 for both). Similarly, the frequency of symptomatic subjects in the p.A341-neighbouring subgroup was intermediate between the other two groups (43% vs. 73% vs. 20%; P < 0.001). These differences in clinical severity can be explained, for p.A341V vs. p.A341-neighbouring mutations, by the p.A341V-specific impairment of IKs regulation. The differences between the p.A341-neighbouring subgroup and the rest of LQT1 mutations may be explained by the functional importance of the S6 segment for channel activation.
Conclusion: KCNQ1 S6 segment mutations surrounding p.A341 increase arrhythmic risk. p.A341V-specific loss of PKA-dependent IKs enhancement correlates with its phenotypic severity. Cellular studies providing further insights into IKs-channel regulation and knowledge of structure-function relationships could improve risk stratification. These findings impact on clinical management.
Keywords: Genetics; Long QT syndrome; Sudden cardiac death.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2021. For permissions, please email: journals.permissions@oup.com.
Figures







Comment in
-
Does knowledge of the mutation in hereditary long QT syndrome aid risk stratification?Eur Heart J. 2021 Dec 7;42(46):4756-4758. doi: 10.1093/eurheartj/ehab668. Eur Heart J. 2021. PMID: 34542608 Free PMC article. No abstract available.
References
-
- Schwartz PJ, Periti M, Malliani A. The long Q-T syndrome. Am Heart J 1975;89:378–390. - PubMed
-
- Schwartz PJ, Ackerman MJ. The long QT syndrome: a transatlantic clinical approach to diagnosis and therapy. Eur Heart J 2013;34:3109–3116. - PubMed
-
- Schwartz PJ. 1970-2020: 50 years of research on the long QT syndrome. From almost zero knowledge to precision medicine. Eur Heart J 2021;42:1063–1072. - PubMed
