

Initial Laparotomy Versus Peritoneal Drainage in Extremely Low Birthweight Infants With Surgical Necrotizing Enterocolitis or Isolated Intestinal Perforation: A Multicenter Randomized Clinical Trial
- PMID: 34506326
- PMCID: PMC8439547
- DOI: 10.1097/SLA.0000000000005099
Initial Laparotomy Versus Peritoneal Drainage in Extremely Low Birthweight Infants With Surgical Necrotizing Enterocolitis or Isolated Intestinal Perforation: A Multicenter Randomized Clinical Trial
Abstract
Objective: The aim of this study was to determine which initial surgical treatment results in the lowest rate of death or neurodevelopmental impairment (NDI) in premature infants with necrotizing enterocolitis (NEC) or isolated intestinal perforation (IP).
Summary background data: The impact of initial laparotomy versus peritoneal drainage for NEC or IP on the rate of death or NDI in extremely low birth weight infants is unknown.
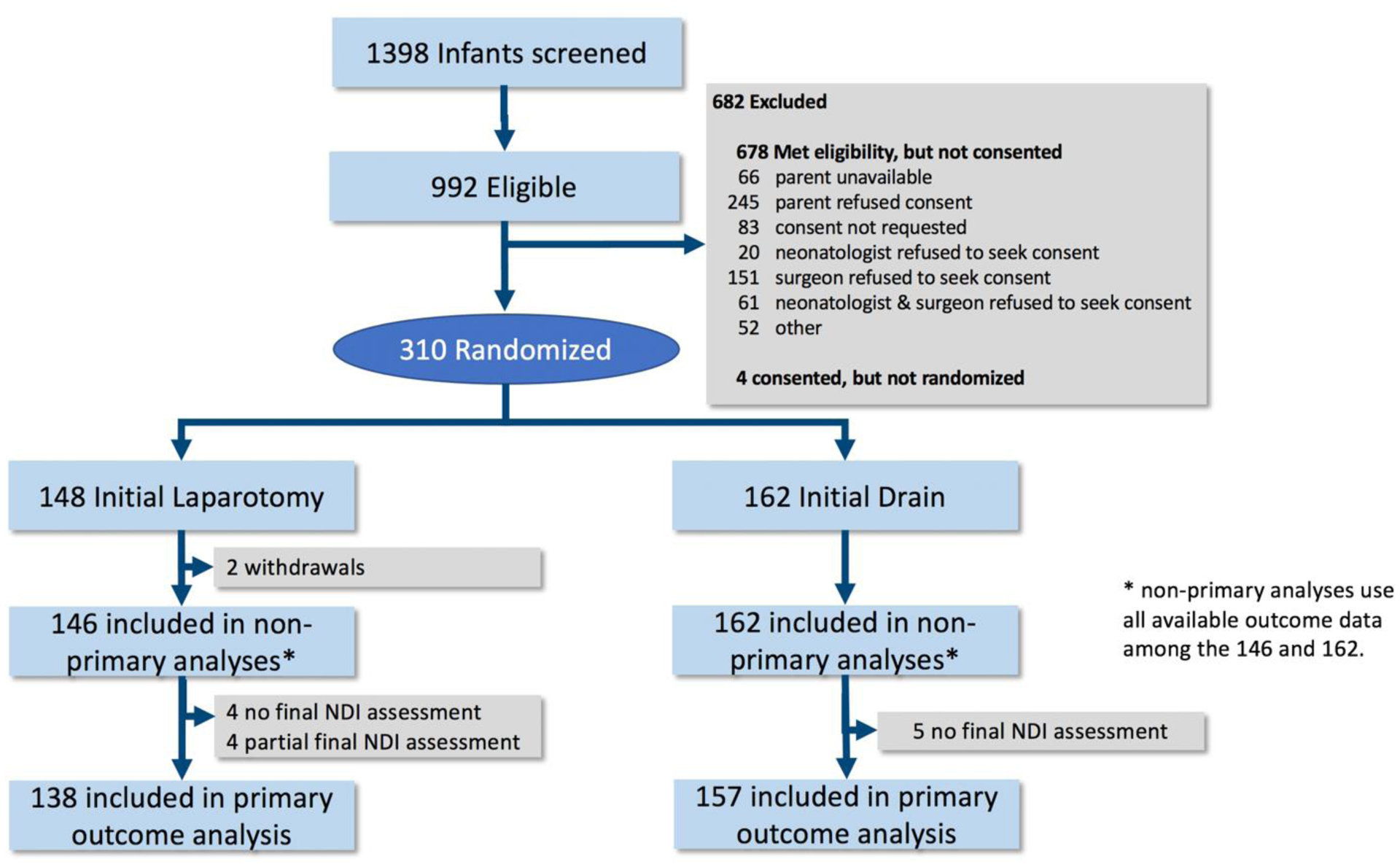
Methods: We conducted the largest feasible randomized trial in 20 US centers, comparing initial laparotomy versus peritoneal drainage. The primary outcome was a composite of death or NDI at 18 to 22 months corrected age, analyzed using prespecified frequentist and Bayesian approaches.
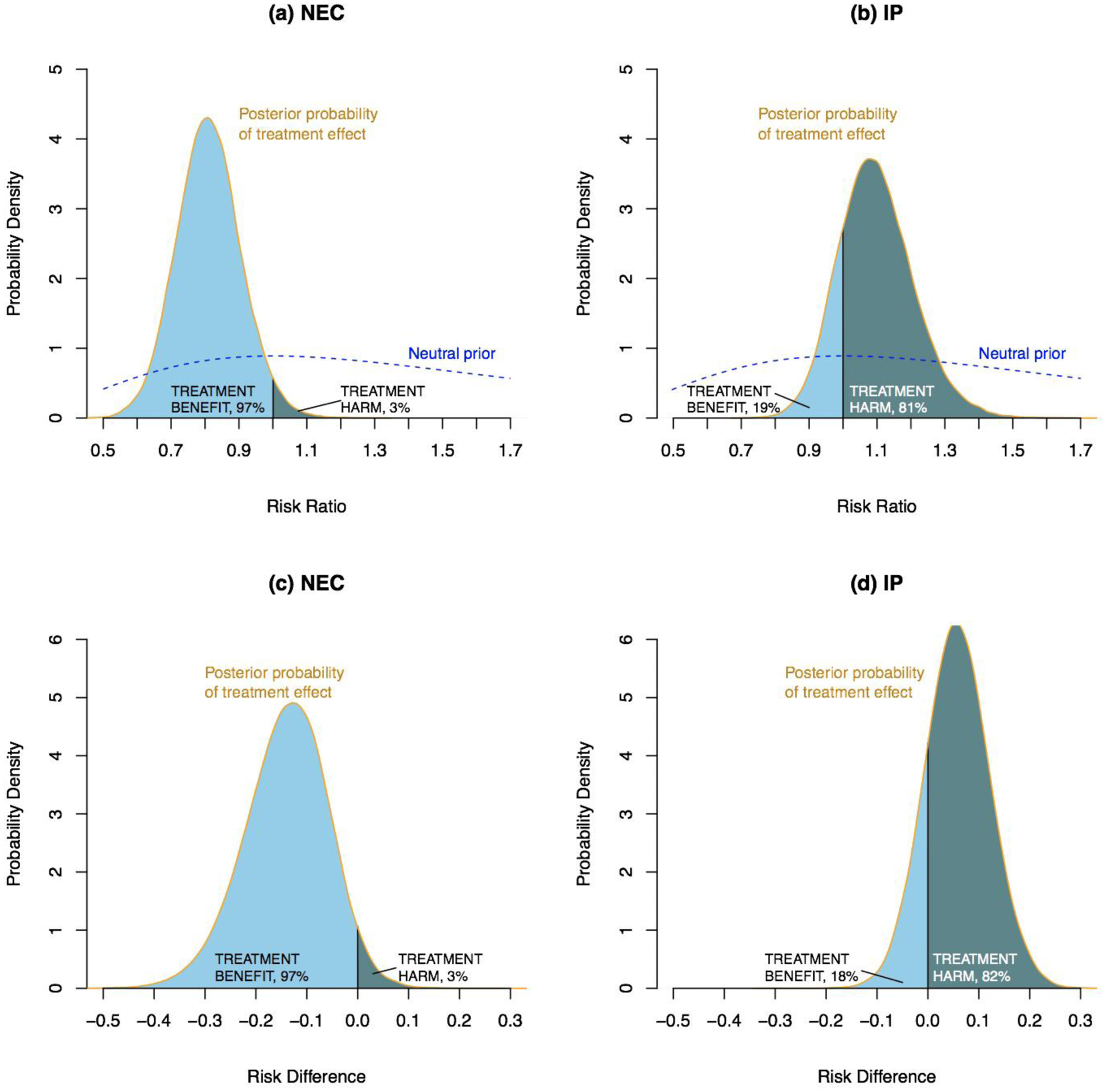
Results: Of 992 eligible infants, 310 were randomized and 96% had primary outcome assessed. Death or NDI occurred in 69% of infants in the laparotomy group versus 70% with drainage [adjusted relative risk (aRR) 1.0; 95% confidence interval (CI): 0.87-1.14]. A preplanned analysis identified an interaction between preoperative diagnosis and treatment group (P = 0.03). With a preoperative diagnosis of NEC, death or NDI occurred in 69% after laparotomy versus 85% with drainage (aRR 0.81; 95% CI: 0.64-1.04). The Bayesian posterior probability that laparotomy was beneficial (risk difference <0) for a preoperative diagnosis of NEC was 97%. For preoperative diagnosis of IP, death or NDI occurred in 69% after laparotomy versus 63% with drainage (aRR, 1.11; 95% CI: 0.95-1.31); Bayesian probability of benefit with laparotomy = 18%.
Conclusions: There was no overall difference in death or NDI rates at 18 to 22 months corrected age between initial laparotomy versus drainage. However, the preoperative diagnosis of NEC or IP modified the impact of initial treatment.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no conflict of interests.
Figures
References
-
- Blakely ML, Tyson JE, Lally KP, et al. Laparotomy versus peritoneal drainage for necrotizing enterocolitis or isolated intestinal perforation in extremely low birth weight infants: outcomes through 18 months adjusted age. Pediatrics 2006; 117(4): e680–687. - PubMed
-
- Hintz SR, Kendrick DE, Stoll BJ, et al. Neurodevelopmental and growth outcomes of extremely low birth weight infants after necrotizing enterocolitis. Pediatrics 2005; 115(3): 696–703. - PubMed
-
- Pumberger W, Mayr M, Kohlhauser C, et al. Spontaneous localized intestinal perforation in very low birth weight infants: a distinct clinical entity different from necrotizing enterocolitis. J Am Coll Surg 2002; 195: 796–803. - PubMed
Publication types
MeSH terms
Grants and funding
- UG1 HD068263/HD/NICHD NIH HHS/United States
- U10 HD021373/HD/NICHD NIH HHS/United States
- UL1 RR025764/RR/NCRR NIH HHS/United States
- UG1 HD027856/HD/NICHD NIH HHS/United States
- UG1 HD034216/HD/NICHD NIH HHS/United States
- UG1 HD027880/HD/NICHD NIH HHS/United States
- UG1 HD053109/HD/NICHD NIH HHS/United States
- UG1 HD027851/HD/NICHD NIH HHS/United States
- U10 HD036790/HD/NICHD NIH HHS/United States
- UL1 TR003142/TR/NCATS NIH HHS/United States
- UG1 HD087226/HD/NICHD NIH HHS/United States
- U10 HD053124/HD/NICHD NIH HHS/United States
- U10 HD053119/HD/NICHD NIH HHS/United States
- U01 HD036790/HD/NICHD NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- UL1 TR002538/TR/NCATS NIH HHS/United States
- UG1 HD068270/HD/NICHD NIH HHS/United States
- UG1 HD068244/HD/NICHD NIH HHS/United States
- UG1 HD027853/HD/NICHD NIH HHS/United States
- UL1 TR000042/TR/NCATS NIH HHS/United States
- UG1 HD087229/HD/NICHD NIH HHS/United States
- UL1 TR003167/TR/NCATS NIH HHS/United States
- UL1 TR000006/TR/NCATS NIH HHS/United States
- UG1 HD040689/HD/NICHD NIH HHS/United States
- UG1 HD053089/HD/NICHD NIH HHS/United States
- UL1 TR000093/TR/NCATS NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- U10 HD027871/HD/NICHD NIH HHS/United States
- UG1 HD027904/HD/NICHD NIH HHS/United States
- UL1 TR000142/TR/NCATS NIH HHS/United States
- UL1 TR000041/TR/NCATS NIH HHS/United States
- UG1 HD068284/HD/NICHD NIH HHS/United States
- UG1 HD021385/HD/NICHD NIH HHS/United States
- UG1 HD040492/HD/NICHD NIH HHS/United States
- UG1 HD021364/HD/NICHD NIH HHS/United States
- UL1 TR001117/TR/NCATS NIH HHS/United States
- UL1 TR000077/TR/NCATS NIH HHS/United States
- UG1 HD068278/HD/NICHD NIH HHS/United States
- U24 HD095254/HD/NICHD NIH HHS/United States
