

Randomized phase 3 ALCANZA study of brentuximab vedotin vs physician's choice in cutaneous T-cell lymphoma: final data
- PMID: 34507350
- PMCID: PMC9153035
- DOI: 10.1182/bloodadvances.2021004710
Randomized phase 3 ALCANZA study of brentuximab vedotin vs physician's choice in cutaneous T-cell lymphoma: final data
Erratum in
-
Horwitz SM, Scarisbrick JJ, Dummer R, et al. Randomized phase 3 ALCANZA study of brentuximab vedotin vs physician's choice in cutaneous T-cell lymphoma: final data. Blood Adv. 2021;5(23):5098-5106.Blood Adv. 2024 May 14;8(9):2243. doi: 10.1182/bloodadvances.2024012976. Blood Adv. 2024. PMID: 38743412 Free PMC article. Clinical Trial. No abstract available.
Abstract
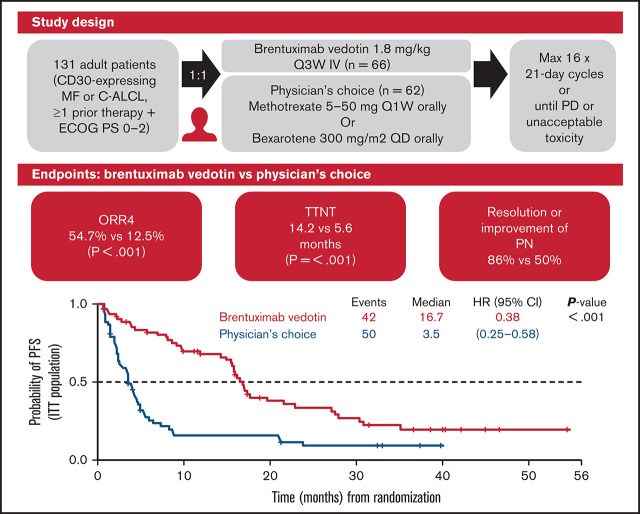
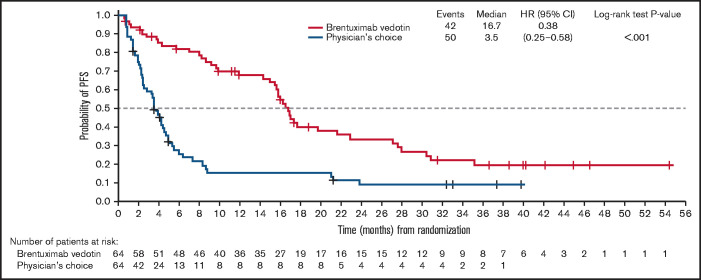
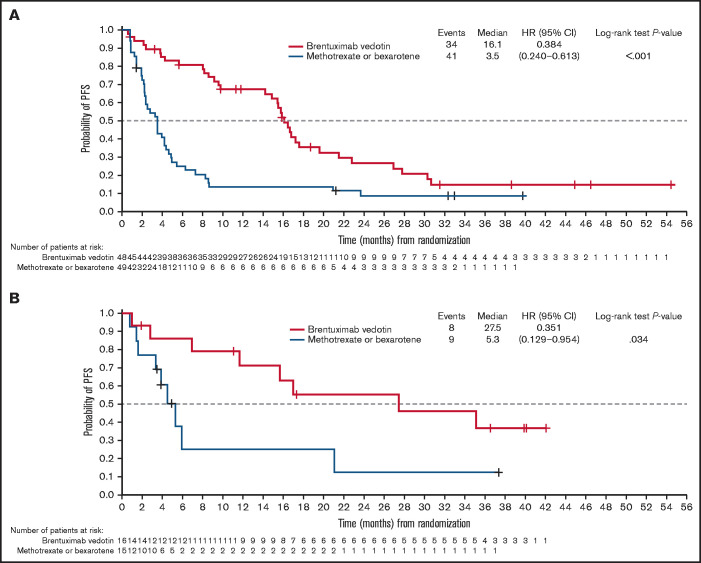
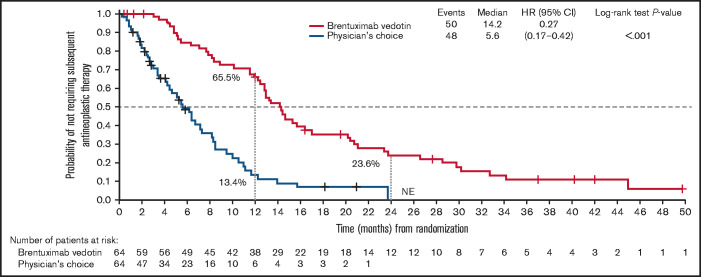
The primary analysis of the phase 3 ALCANZA trial showed significantly improved objective responses lasting ≥4 months (ORR4; primary endpoint) and progression-free survival (PFS) with brentuximab vedotin vs physician's choice (methotrexate or bexarotene) in CD30-expressing mycosis fungoides (MF) or primary cutaneous anaplastic large-cell lymphoma (C-ALCL). Cutaneous T-cell lymphomas often cause pruritus and pain; brentuximab vedotin improved skin symptom burden with no negative effects on quality of life. We report final data from ALCANZA (median follow-up, 45.9 months). Adults with previously treated CD30-expressing MF/C-ALCL were randomly assigned to brentuximab vedotin (n = 64) or physician's choice (n = 64). Final data demonstrated improved responses per independent review facility with brentuximab vedotin vs physician's choice: ORR4; 54.7% vs 12.5% (P < .001); complete response, 17.2% vs 1.6% (P = .002). Median PFS with brentuximab vedotin vs physician's choice was 16.7 months vs 3.5 months (P < .001). Median time to the next treatment was significantly longer with brentuximab vedotin than with physician's choice (14.2 vs 5.6 months; hazard ratio, 0.27; 95% confidence interval, 0.17-0.42; P < .001). Of 44 patients in the brentuximab vedotin arm who experienced any-grade peripheral neuropathy, (grade 3, n = 6; grade 4, n = 0), 86% (38 of 44) had complete resolution (26 of 44) or improvement to grades 1 and 2 (12 of 44). Peripheral neuropathy was ongoing in 18 patients (all grades 1-2). These final analyses confirm improved, clinically meaningful, durable responses and longer PFS with brentuximab vedotin vs physician's choice in CD30-expressing MF or C-ALCL. This trial was registered at https://www.clinicaltrials.gov as #NCT01578499.
© 2021 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Figures
References
-
- Willemze R, Hodak E, Zinzani PL, Specht L, Ladetto M; ESMO Guidelines Committee . Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29(suppl 4):iv30-iv40. - PubMed
-
- Zinzani PL, Bonthapally V, Huebner D, Lutes R, Chi A, Pileri S. Panoptic clinical review of the current and future treatment of relapsed/refractory T-cell lymphomas: peripheral T-cell lymphomas. Crit Rev Oncol Hematol. 2016;99:214-227. - PubMed
-
- Kartan S, Johnson WT, Sokol K, et al. The spectrum of CD30+ T cell lymphoproliferative disorders in the skin. Chi Clin Oncol. 2019; 8(1):3. - PubMed
-
- Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105(10):3768-3785. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
