

Severe hypertension in pregnancy
- PMID: 34507929
- PMCID: PMC8439512
- DOI: 10.7861/clinmed.2021-0508
Severe hypertension in pregnancy
Abstract
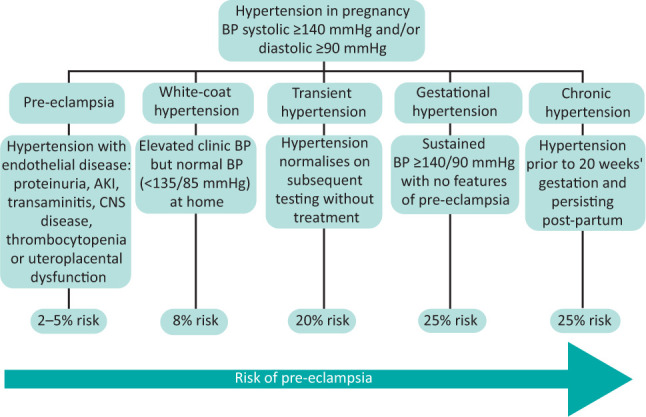
Severe hypertension in pregnancy is defined as a sustained systolic blood pressure of 160 mmHg or over or diastolic blood pressure of 110 mmHg or over and should be assessed in hospital. Severe hypertension before 20 weeks' gestation is rare and usually due to chronic hypertension; assessment for target organ damage and exclusion of secondary hypertension are warranted. The most common cause of severe hypertension in pregnancy is pre-eclampsia, which presents after 20 weeks' gestation. This warrants more rapid control of blood pressure due to the risk of haemorrhagic stroke, and intravenous antihypertensive agents may be required. Treatment is determined by licensing, availability and clinician experience, with no high-level evidence to guide prescribing. Labetalol is the agent most commonly used, both orally and intravenously, in pregnancy in the UK. Severe hypertension is a risk factor for sustained hypertension after pregnancy. Hypertension in pregnancy is associated with increased cardiovascular risk.
Keywords: hypertension; pre-eclampsia; pregnancy.
© Royal College of Physicians 2021. All rights reserved.
Figures
References
-
- Green LJ, Mackillop LH, Salvi D, et al. Gestation-specific vital sign reference ranges in pregnancy. Obstet Gynecol 2020;135:653–64. - PubMed
-
- Martin JN, Thigpen BD, Moore RC, et al. Stroke and severe preeclampsia and eclampsia: a paradigm shift focusing on systolic blood pressure. Obstet Gynecol 2005;105:246–54. - PubMed
-
- Lewis G. (ed). Saving mothers’ lives: reviewing maternal deaths to make motherhood safer –2003–2005. Confidential Enquiry into Maternal and Child Health, 2007. www.publichealth.hscni.net/publications/saving-mothers-lives-2003-2005 [Accessed 28 July 2021].
-
- Brown MA, Magee LA, Kenny LC, et al. International Society for the Study of Hypertension in Pregnancy (ISSHP). Hypertensive disorders of pregnancy: ISSHP classification, diagnosis, and management recommendations for international practice. Hypertension 2018;72:24–43. - PubMed
-
- Wiles K, Brown M. Renal physiology and complications in normal pregnancy. In Comprehensive clinical nephrology, 7th edn. Elsevier, 2021: in press.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
