

Association of MAFLD With Diabetes, Chronic Kidney Disease, and Cardiovascular Disease: A 4.6-Year Cohort Study in China
- PMID: 34508601
- PMCID: PMC8684479
- DOI: 10.1210/clinem/dgab641
Association of MAFLD With Diabetes, Chronic Kidney Disease, and Cardiovascular Disease: A 4.6-Year Cohort Study in China
Abstract
Context: In 2020, the terminology of metabolic dysfunction-associated fatty liver disease (MAFLD) was proposed to replace nonalcoholic fatty liver disease (NAFLD).
Objectives: This work aimed to investigate the prevalence and incidence of MAFLD and evaluate its effects on incident extrahepatic diseases.
Methods: A total of 6873 individuals, with a 4.6-year follow-up, were included in this study. Associations of MAFLD and NAFLD with diabetes, chronic kidney disease (CKD), and cardiovascular disease (CVD) were examined using logistic regression and Cox proportional hazards models.
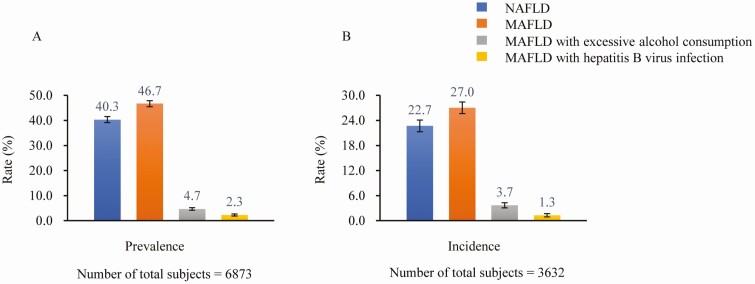
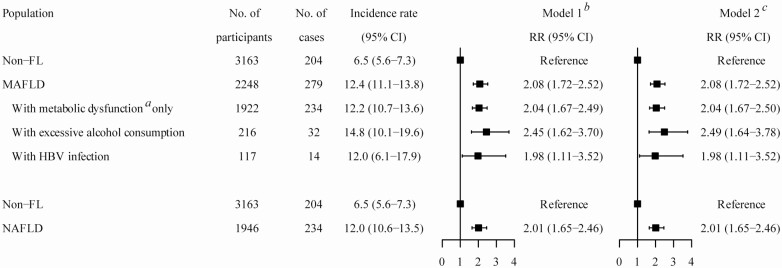
Results: The prevalence of NAFLD and MAFLD was 40.3% (95% CI, 39.2%-41.5%) and 46.7% (95% CI, 45.6%-47.9%), respectively. Additionally, 321 (4.7%) and 156 (2.3%) participants had MAFLD with excessive alcohol consumption and hepatitis B virus (HBV) infection. During the follow-up period, the incidence of NAFLD and MAFLD was 22.7% (95% CI, 21.3%-24.0%) and 27.0% (95% CI, 25.5%-28.4%). MAFLD was associated with higher risks of incident diabetes (risk ratio [RR] 2.08; 95% CI, 1.72-2.52), CKD (RR 1.64; 95% CI, 1.39-1.94), and CVD (hazard ratio 1.44; 95% CI, 1.15-1.81). Similar associations for NAFLD were observed. Furthermore, the MAFLD subgroups with excessive alcohol consumption (RR 2.49; 95% CI, 1.64-3.78) and HBV infection (RR 1.98; 95% CI, 1.11-3.52) were associated with higher risks of incident diabetes.
Conclusion: The change from NAFLD to MAFLD did not greatly affect the associations with diabetes, CKD, and CVD. MAFLD further identified those patients of metabolically fatty liver combined with excessive alcohol consumption and HBV infection, who had increased risks of incident diabetes compared with those of non-fatty liver.
Keywords: cardiovascular disease; chronic kidney disease; diabetes; metabolic dysfunction–associated fatty liver disease; nonalcoholic fatty liver disease.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Endocrine Society.
Figures


References
-
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease—meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73-84. - PubMed
-
- Zhou F, Zhou J, Wang W, et al. Unexpected rapid increase in the burden of NAFLD in China from 2008 to 2018: a systematic review and meta-analysis. Hepatology. 2019;70(4):1119-1133. - PubMed
-
- Choi HSJ, Brouwer WP, Zanjir WMR, et al. Nonalcoholic steatohepatitis is associated with liver-related outcomes and all-cause mortality in chronic hepatitis B. Hepatology. 2020;71(2):539-548. - PubMed
-
- Eslam M, Newsome PN, Sarin SK, et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol. 2020;73(1):202-209. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
