

Immunologic resilience and COVID-19 survival advantage
- PMID: 34508765
- PMCID: PMC8425719
- DOI: 10.1016/j.jaci.2021.08.021
Immunologic resilience and COVID-19 survival advantage
Abstract
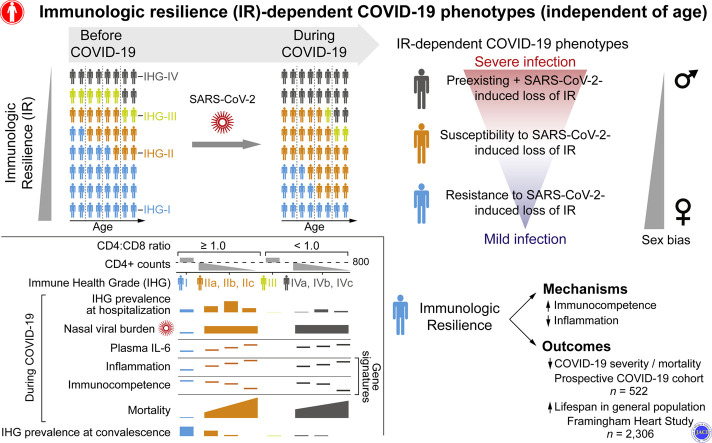
Background: The risk of severe coronavirus disease 2019 (COVID-19) varies significantly among persons of similar age and is higher in males. Age-independent, sex-biased differences in susceptibility to severe COVID-19 may be ascribable to deficits in a sexually dimorphic protective attribute that we termed immunologic resilience (IR).
Objective: We sought to examine whether deficits in IR that antedate or are induced by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection independently predict COVID-19 mortality.
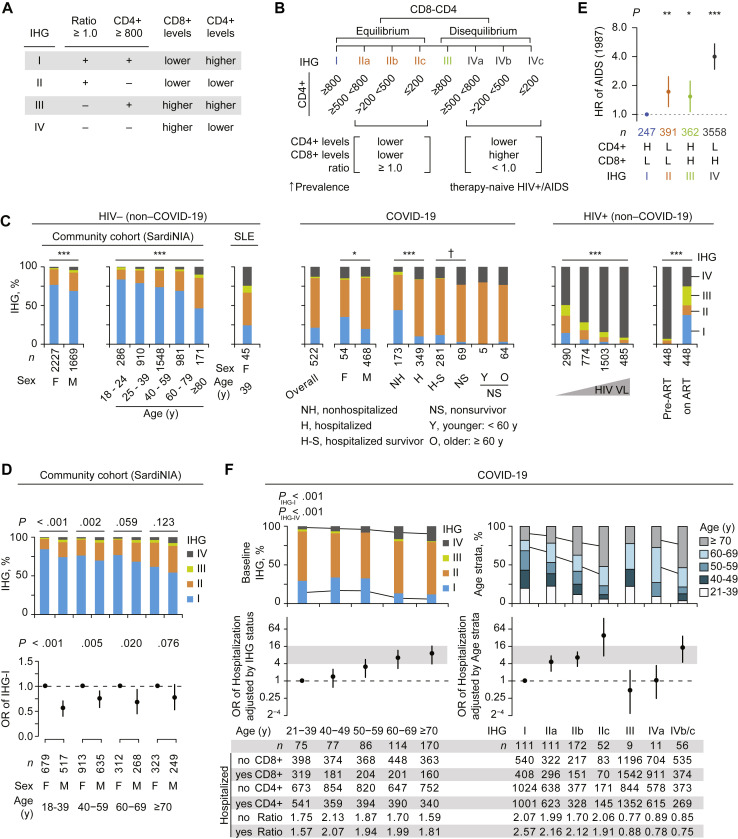
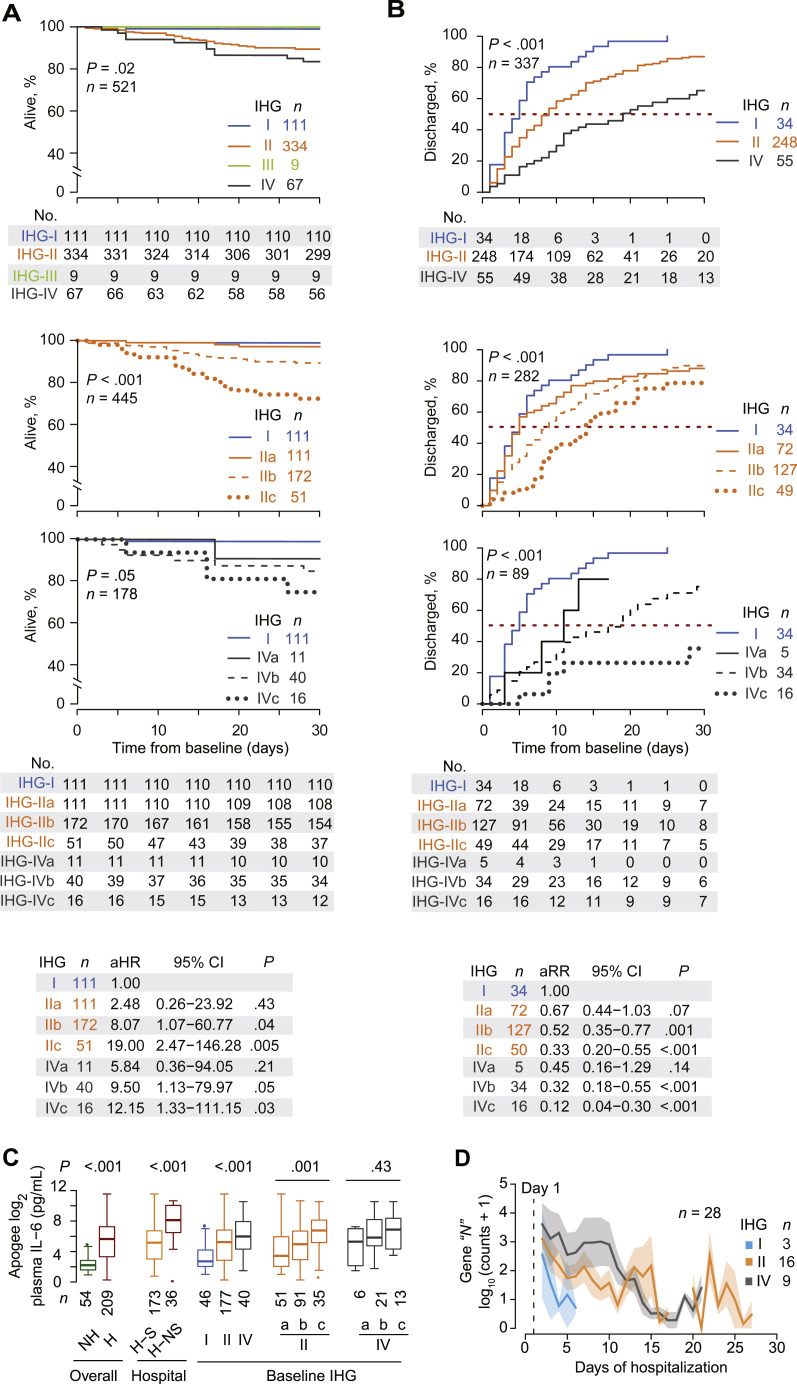
Methods: IR levels were quantified with 2 novel metrics: immune health grades (IHG-I [best] to IHG-IV) to gauge CD8+ and CD4+ T-cell count equilibrium, and blood gene expression signatures. IR metrics were examined in a prospective COVID-19 cohort (n = 522); primary outcome was 30-day mortality. Associations of IR metrics with outcomes in non-COVID-19 cohorts (n = 13,461) provided the framework for linking pre-COVID-19 IR status to IR during COVID-19, as well as to COVID-19 outcomes.
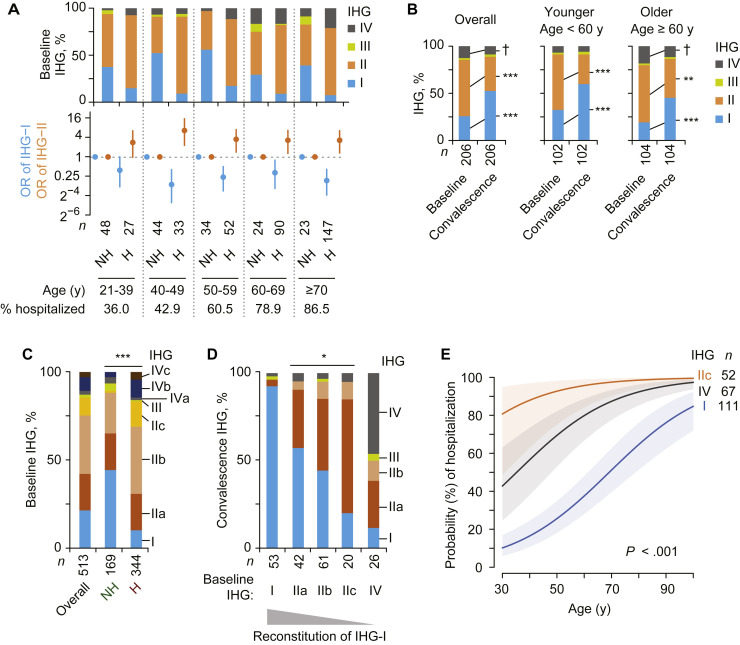
Results: IHG-I, tracking high-grade equilibrium between CD8+ and CD4+ T-cell counts, was the most common grade (73%) among healthy adults, particularly in females. SARS-CoV-2 infection was associated with underrepresentation of IHG-I (21%) versus overrepresentation (77%) of IHG-II or IHG-IV, especially in males versus females (P < .01). Presentation with IHG-I was associated with 88% lower mortality, after controlling for age and sex; reduced risk of hospitalization and respiratory failure; lower plasma IL-6 levels; rapid clearance of nasopharyngeal SARS-CoV-2 burden; and gene expression signatures correlating with survival that signify immunocompetence and controlled inflammation. In non-COVID-19 cohorts, IR-preserving metrics were associated with resistance to progressive influenza or HIV infection, as well as lower 9-year mortality in the Framingham Heart Study, especially in females.
Conclusions: Preservation of immunocompetence with controlled inflammation during antigenic challenges is a hallmark of IR and associates with longevity and AIDS resistance. Independent of age, a male-biased proclivity to degrade IR before and/or during SARS-CoV-2 infection predisposes to severe COVID-19.
Keywords: AIDS; Aging; COVID-19; HIV; SARS-CoV-2; biomarkers; immune; inflammation; influenza.
Published by Elsevier Inc.
Figures
Comment in
-
Immune health grades: Finding resilience in the COVID-19 pandemic and beyond.J Allergy Clin Immunol. 2022 Feb;149(2):565-568. doi: 10.1016/j.jaci.2021.10.025. Epub 2021 Nov 2. J Allergy Clin Immunol. 2022. PMID: 34740606 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
