

Cardiorespiratory Abnormalities in Patients Recovering from Coronavirus Disease 2019
- PMID: 34508837
- PMCID: PMC8425293
- DOI: 10.1016/j.echo.2021.08.022
Cardiorespiratory Abnormalities in Patients Recovering from Coronavirus Disease 2019
Abstract
Background: A large number of patients around the world are recovering from coronavirus disease 2019 (COVID-19); many of them report persistence of symptoms. The aim of this study was to test pulmonary, cardiovascular, and peripheral responses to exercise in patients recovering from COVID-19.
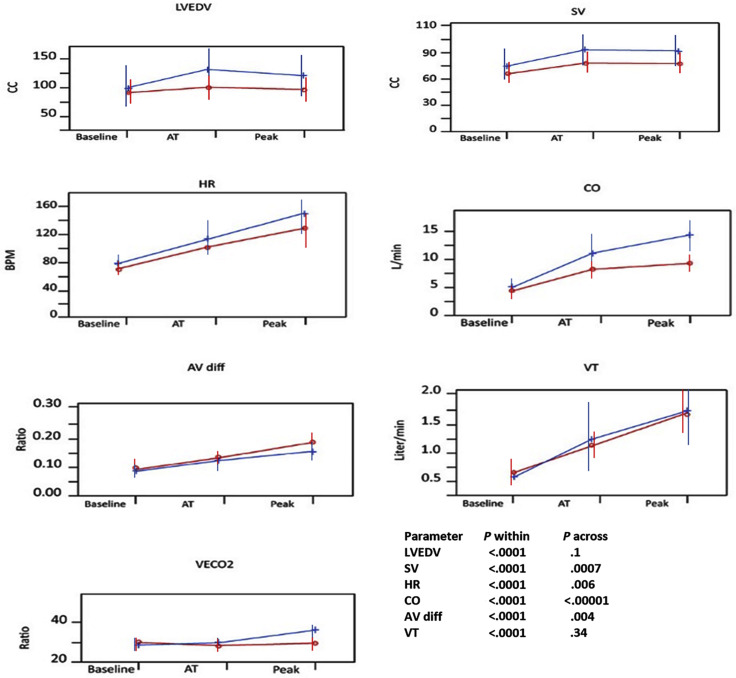
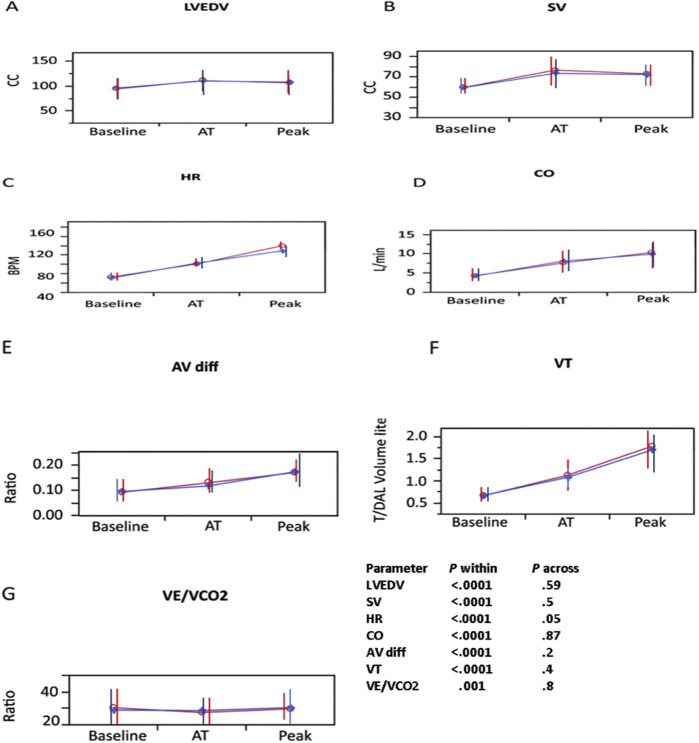
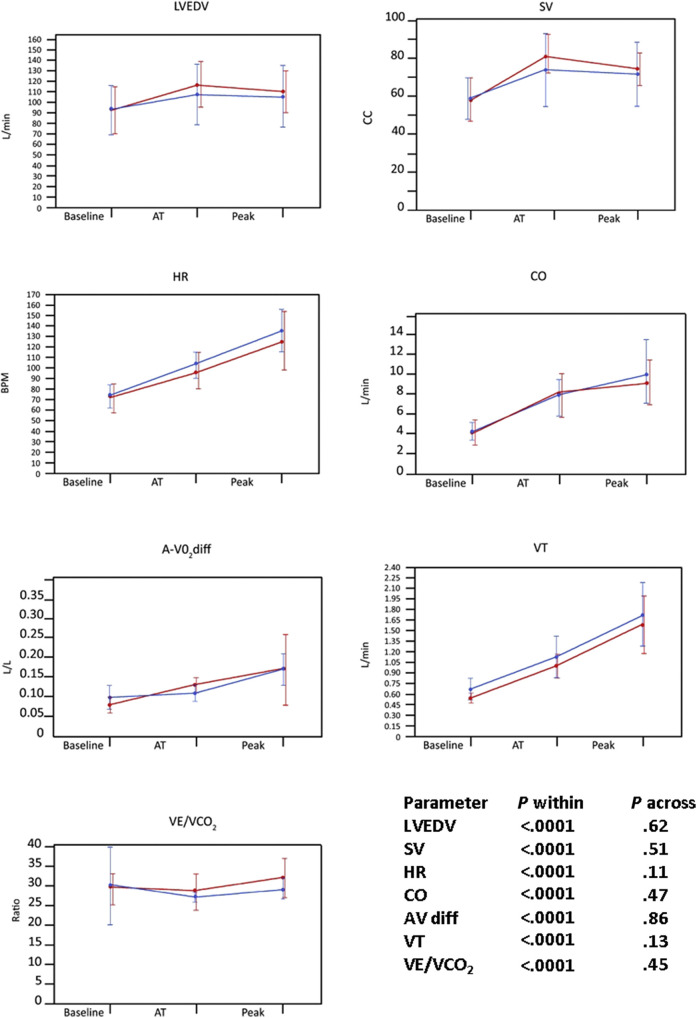
Methods: Patients who recovered from COVID-19 were prospectively evaluated using a combined anatomic and functional assessment. All patients underwent clinical examination, laboratory tests, and combined stress echocardiography and cardiopulmonary exercise testing. Left ventricular volumes, ejection fraction, stroke volume, heart rate, E/e' ratio, right ventricular function, oxygen consumption (Vo2), lung volumes, ventilatory efficiency, oxygen saturation, and muscle oxygen extraction were measured in all effort stages and compared with values in historical control subjects.
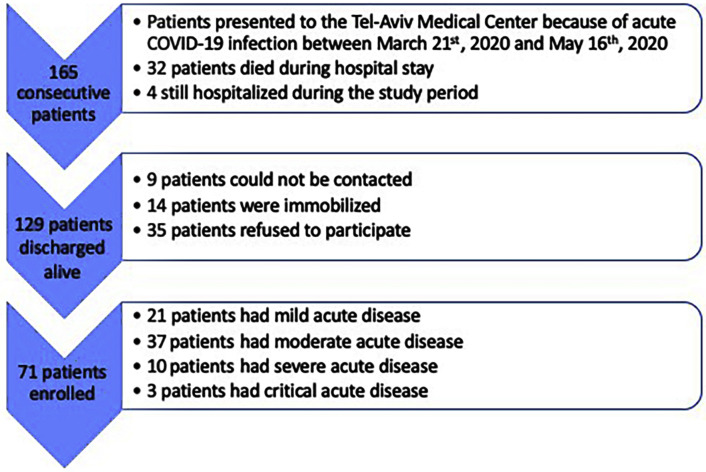
Results: A total of 71 patients were assessed 90.6 ± 26 days after the onset of COVID-19 symptoms. Only 23 (33%) were asymptomatic. The most common symptoms were fatigue (34%), muscle weakness or pain (27%), and dyspnea (22%). Vo2 was lower among post-COVID-19 patients compared with control subjects (P = .03, group-by-time interaction P = .007). Reduction in peak Vo2 was due to a combination of chronotropic incompetence (75% of post-COVID-19 patients vs 8% of control subjects, P < .0001) and an insufficient increase in stroke volume during exercise (P = .0007, group-by-time interaction P = .03). Stroke volume limitation was mostly explained by diminished increase in left ventricular end-diastolic volume (P = .10, group-by-time interaction P = .03) and insufficient increase in ejection fraction (P = .01, group-by-time interaction P = .01). Post-COVID-19 patients had higher peripheral oxygen extraction (P = .004) and did not have significantly different respiratory and gas exchange parameters compared with control subjects.
Conclusions: Patients recovering from COVID-19 have symptoms associated with objective reduction in peak Vo2. The mechanism of this reduction is complex and mainly involves a combination of attenuated heart rate and stroke volume reserve.
Keywords: COVID-19; Cardiopulmonary exercise test; Long COVID; Post-COVID; Stress echocardiography.
Copyright © 2021 American Society of Echocardiography. Published by Elsevier Inc. All rights reserved.
Figures

References
Supplemental References
-
- Nagueh S.F., Smiseth O.A., Appleton C.P., Byrd B.F., III, Dokainish H., Edvardsen T., et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2016;17:1321–1360. - PubMed
-
- Lang R.M., Badano L.P., Mor-Avi V., Afilalo J., Armstrong A., Ernande L., et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28:1–39.e14. - PubMed
-
- Topilsky Y., Khanna A.D., Oh J.K., Nishimura R.A., Enriquez-Sarano M., Jeon Y.B., et al. Preoperative factors associated with adverse outcome after tricuspid valve replacement. Circulation. 2011;123:1929–1939. - PubMed
-
- Kitabatake A., Inoue M., Asao M., Masuyama T., Tanouchi J., Morita T., et al. Noninvasive evaluation of pulmonary hypertension by a pulsed Doppler technique. Circulation. 1983;68:302–309. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
