

SARS-CoV2-specific Humoral and T-cell Immune Response After Second Vaccination in Liver Cirrhosis and Transplant Patients
- PMID: 34509643
- PMCID: PMC8427908
- DOI: 10.1016/j.cgh.2021.09.003
SARS-CoV2-specific Humoral and T-cell Immune Response After Second Vaccination in Liver Cirrhosis and Transplant Patients
Abstract
Background & aims: Detailed information on the immune response after second vaccination of cirrhotic patients and liver transplant (LT) recipients against severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2) is largely missing. We aimed at comparing the vaccine-induced humoral and T-cell responses of these vulnerable patient groups.
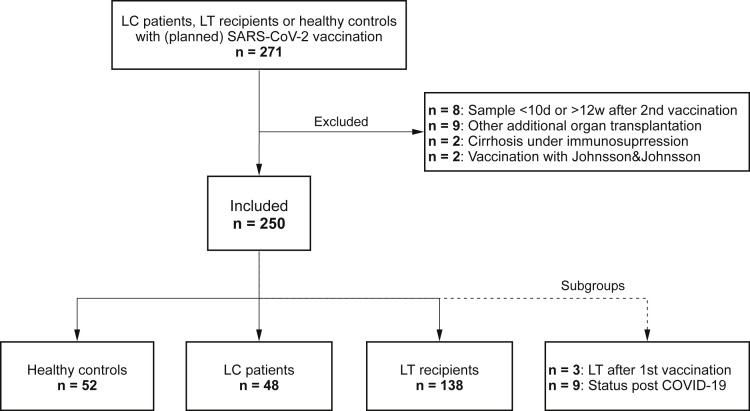
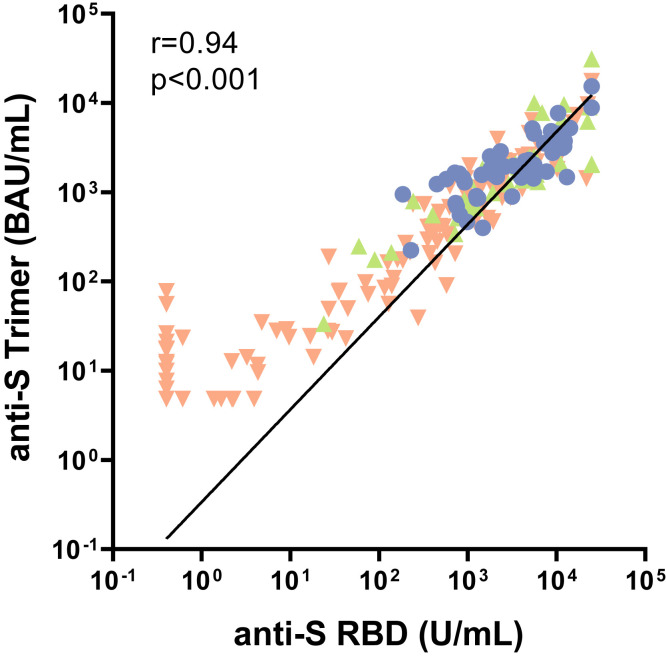
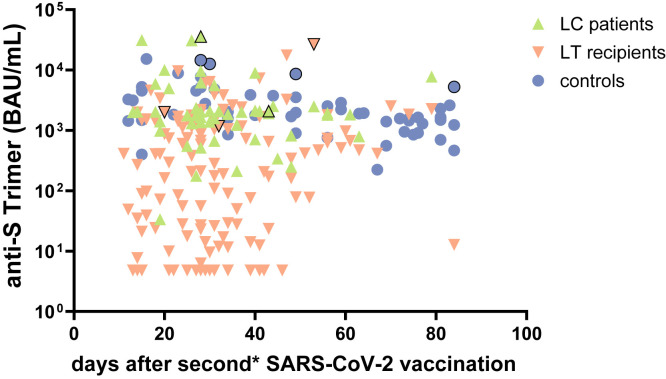
Methods: In this prospective cohort study, anti-SARS-CoV-2 spike-protein titers were determined using the DiaSorin LIAISON (anti-S trimer) and Roche Elecsys (anti-S RBD) immunoassays in 194 patients (141 LT, 53 cirrhosis Child-Pugh A-C) and 56 healthy controls before and 10 to 84 days after second vaccination. The spike-specific T-cell response was assessed using an interferon-gamma release assay (EUROIMMUN). A logistic regression analysis was performed to identify predictors of low response.
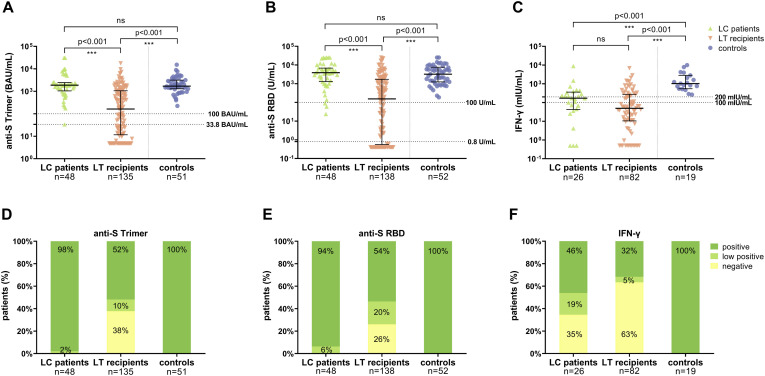
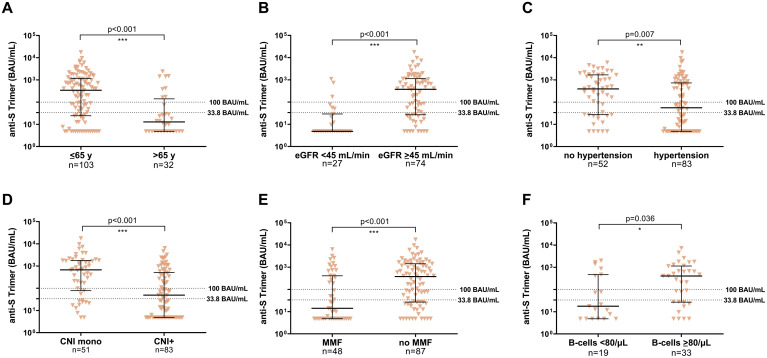
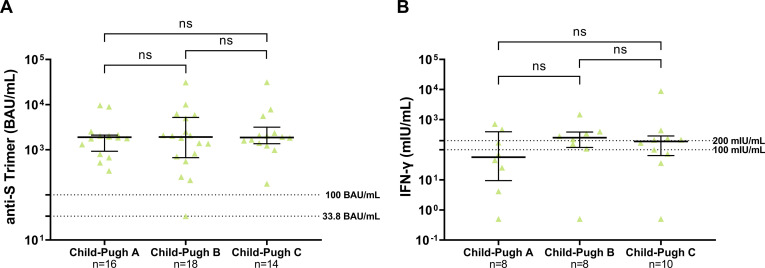
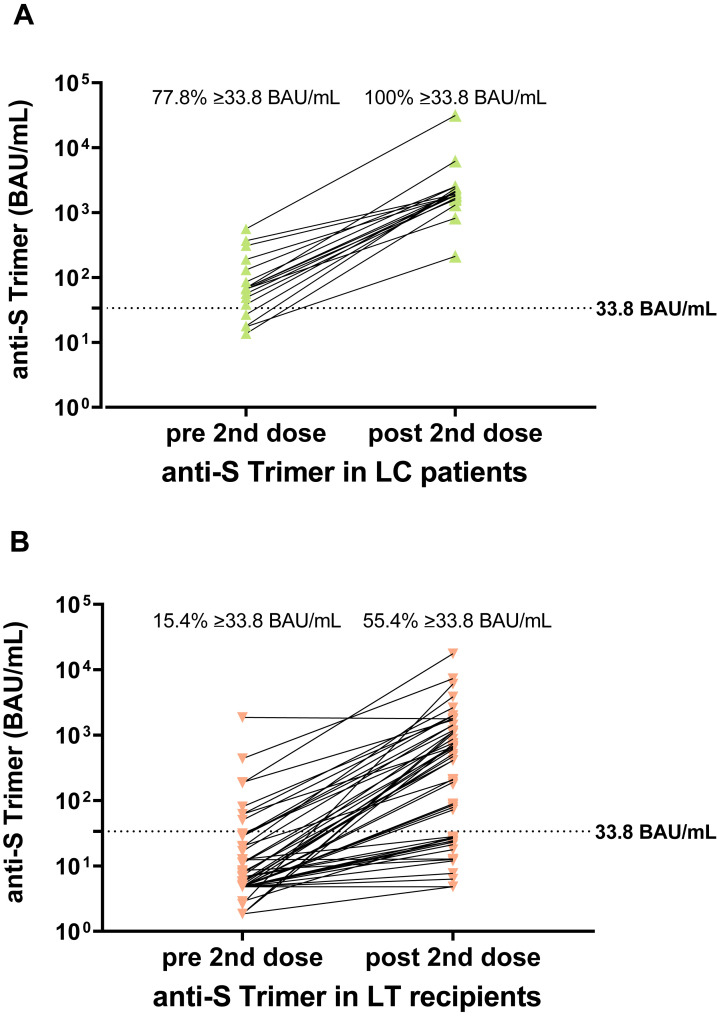
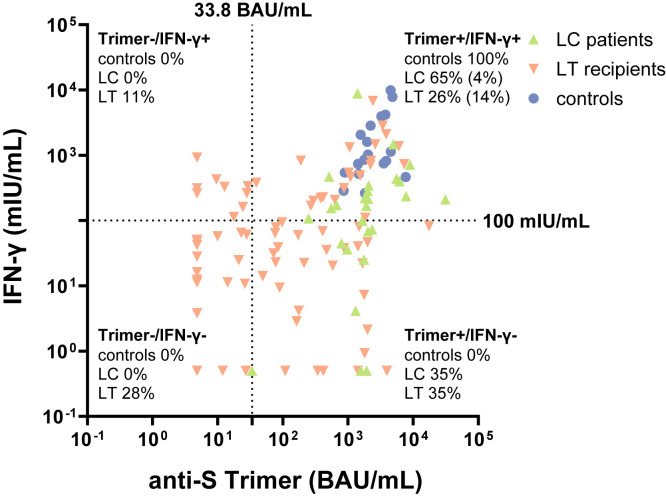
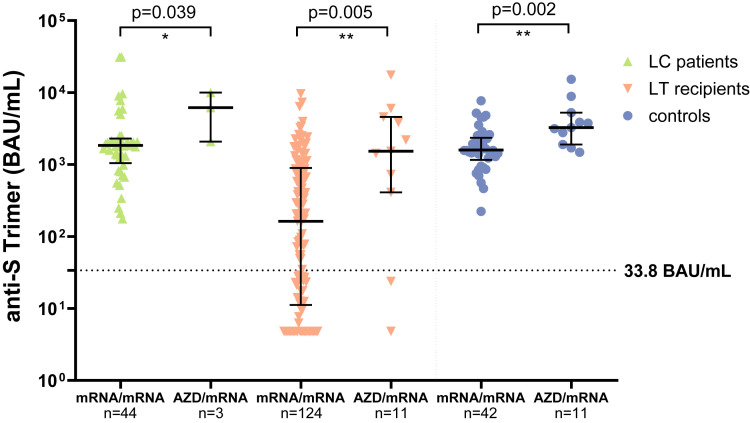
Results: After the second vaccination, seroconversion was achieved in 63% of LT recipients and 100% of cirrhotic patients and controls using the anti-S trimer assay. Median anti-SARS-CoV-2 titers of responding LT recipients were lower compared with cirrhotic patients and controls (P < .001). Spike-specific T-cell response rates were 36.6%, 65.4%, and 100% in LT, cirrhosis, and controls, respectively. Altogether, 28% of LT recipients did neither develop a humoral nor a T-cell response after second vaccination. In LT recipients, significant predictors of absent or low humoral response were age >65 years (odds ratio [OR], 4.57; 95% confidence interval [CI], 1.48-14.05) and arterial hypertension (OR, 2.50; 95% CI, 1.10-5.68), whereas vaccination failure was less likely with calcineurin inhibitor monotherapy than with other immunosuppressive regimens (OR, 0.36; 95% CI, 0.13-0.99).
Conclusion: Routine serological testing of the vaccination response and a third vaccination in patients with low or absent response seem advisable. These vulnerable cohorts need further research on the effects of heterologous vaccination and intermittent reduction of immunosuppression before booster vaccinations.
Keywords: Immunosuppression; Liver Cirrhosis; Liver Transplant Recipients; SARS-CoV-2 Vaccination.
Copyright © 2022. Published by Elsevier Inc.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
