

Comparison of the real-world effectiveness of vertical versus lateral functional hemispherotomy techniques for pediatric drug-resistant epilepsy: A post hoc analysis of the HOPS study
- PMID: 34510448
- PMCID: PMC9290517
- DOI: 10.1111/epi.17021
Comparison of the real-world effectiveness of vertical versus lateral functional hemispherotomy techniques for pediatric drug-resistant epilepsy: A post hoc analysis of the HOPS study
Abstract
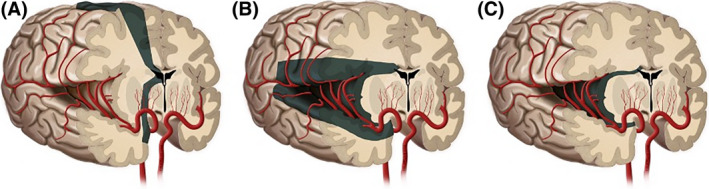
Objective: This study was undertaken to determine whether the vertical parasagittal approach or the lateral peri-insular/peri-Sylvian approach to hemispheric surgery is the superior technique in achieving long-term seizure freedom.
Methods: We conducted a post hoc subgroup analysis of the HOPS (Hemispheric Surgery Outcome Prediction Scale) study, an international, multicenter, retrospective cohort study that identified predictors of seizure freedom through logistic regression modeling. Only patients undergoing vertical parasagittal, lateral peri-insular/peri-Sylvian, or lateral trans-Sylvian hemispherotomy were included in this post hoc analysis. Differences in seizure freedom rates were assessed using a time-to-event method and calculated using the Kaplan-Meier survival method.
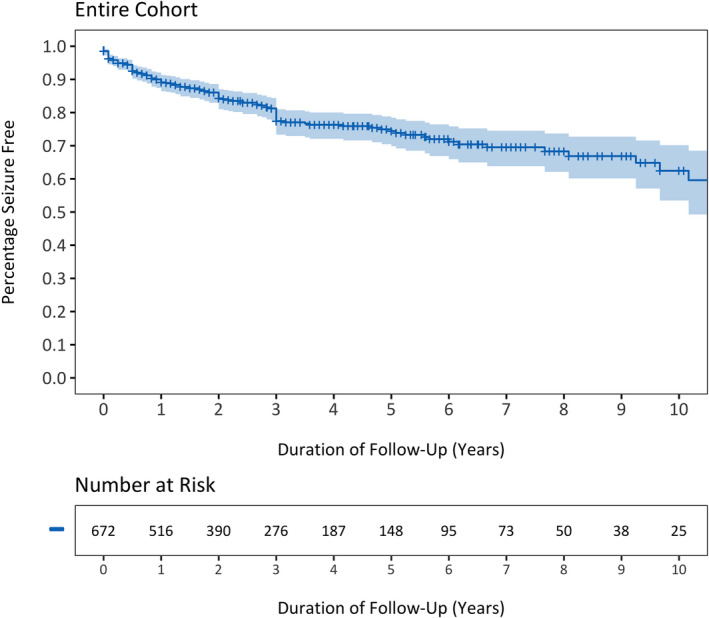
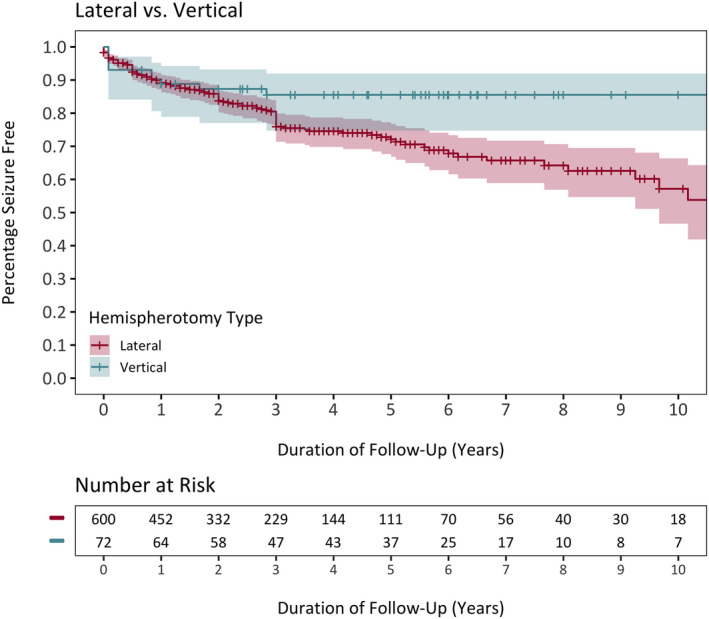
Results: Data for 672 participants across 23 centers were collected on the specific hemispherotomy approach. Of these, 72 (10.7%) underwent vertical parasagittal hemispherotomy and 600 (89.3%) underwent lateral peri-insular/peri-Sylvian or trans-Sylvian hemispherotomy. Seizure freedom was obtained in 62.4% (95% confidence interval [CI] = 53.5%-70.2%) of the entire cohort at 10-year follow-up. Seizure freedom was 88.8% (95% CI = 78.9%-94.3%) at 1-year follow-up and persisted at 85.5% (95% CI = 74.7%-92.0%) across 5- and 10-year follow-up in the vertical subgroup. In contrast, seizure freedom decreased from 89.2% (95% CI = 86.3%-91.5%) at 1-year to 72.1% (95% CI = 66.9%-76.7%) at 5-year to 57.2% (95% CI = 46.6%-66.4%) at 10-year follow-up for the lateral subgroup. Log-rank test found that vertical hemispherotomy was associated with durable seizure-free progression compared to the lateral approach (p = .01). Patients undergoing the lateral hemispherotomy technique had a shorter time-to-seizure recurrence (hazard ratio = 2.56, 95% CI = 1.08-6.04, p = .03) and increased seizure recurrence odds (odds ratio = 3.67, 95% CI = 1.05-12.86, p = .04) compared to those undergoing the vertical hemispherotomy technique.
Significance: This pilot study demonstrated more durable seizure freedom of the vertical technique compared to lateral hemispherotomy techniques. Further studies, such as prospective expertise-based observational studies or a randomized clinical trial, are required to determine whether a vertical approach to hemispheric surgery provides superior long-term seizure outcomes.
Keywords: hemispherectomy; hemispherotomy; seizure outcomes; technique.
© 2021 The Authors. Epilepsia published by Wiley Periodicals LLC on behalf of International League Against Epilepsy.
Conflict of interest statement
G.W.M. is partly supported by the Davies/Crandall Endowed Chair for epilepsy research at University of California, Los Angeles. The views expressed in this article are not the official positions of any author's affiliated institution. P.L.P. has received research support from the National Institutes of Health (NIH), National Science Foundation (NSF), and Boston Healthcare Associates; has received royalty payments from Elsevier, Springer Publishing, and UpToDate; has served as a consultant for Agilis Biotherapeutics and GLG Health Care Council; and is an associate editor for the
Figures
Comment in
-
Vertical hemispherotomy for drug-resistant epilepsy: Toward confirmation of the HOPS study.Epilepsia. 2021 Dec;62(12):3150-3151. doi: 10.1111/epi.17111. Epub 2021 Oct 30. Epilepsia. 2021. PMID: 34716924 No abstract available.
References
-
- Perry MS, Duchowny M. Surgical management of intractable childhood epilepsy: curative and palliative procedures. Semin Pediatr Neurol. 2011;18:195–202. - PubMed
-
- Bailet LL, Turk WR. The impact of childhood epilepsy on neurocognitive and behavioral performance: a prospective longitudinal study. Epilepsia. 2000;41:426–31. - PubMed
-
- Moosa AN, Gupta A, Jehi L, Marashly A, Cosmo G, Lachhwani D, et al. Longitudinal seizure outcome and prognostic predictors after hemispherectomy in 170 children. Neurology. 2013;15(80):253–60. - PubMed
-
- Griessenauer CJ, Salam S, Hendrix P, Patel DM, Tubbs RS, Blount JP, et al. Hemispherectomy for treatment of refractory epilepsy in the pediatric age group: a systematic review. J Neurosurg Pediatr. 2015;15:34–44. - PubMed
-
- McKenzie K. The present status of a patient who had right cerebral hemisphere removed. JAMA. 1938;111:168.
