

Partial uncinatectomy combined with anterior cervical discectomy and fusion for the treatment of one-level cervical radiculopathy: analysis of clinical efficacy and sagittal alignment
- PMID: 34511102
- PMCID: PMC8436428
- DOI: 10.1186/s12891-021-04680-0
Partial uncinatectomy combined with anterior cervical discectomy and fusion for the treatment of one-level cervical radiculopathy: analysis of clinical efficacy and sagittal alignment
Abstract
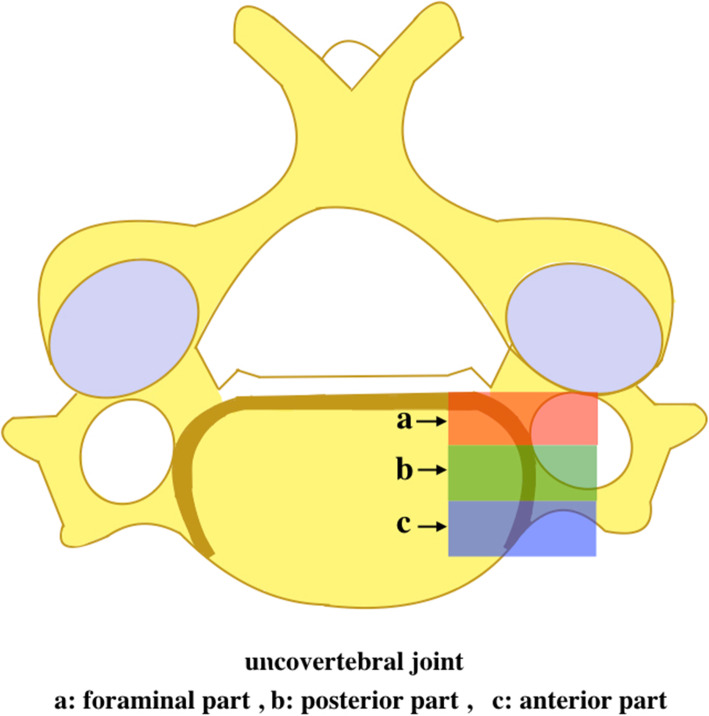
Background: Biomechanical studies have demonstrated that uncovertebral joint contributes to segment mobility and stability to a certain extent. Simultaneously, osteophytes arising from the uncinate process are a common cause of cervical spondylotic radiculopathy (CSR). For such patients, partial uncinatectomy (UT) may be required. However, the clinical efficacy and sagittal alignment of partial UT during anterior cervical discectomy and fusion (ACDF) have not been fully elucidated.
Methods: A total of 87 patients who had undergone single level ACDF using a zero-profile device from July 2014 to December 2018 were included. Based on whether the foraminal part of the uncovertebral joint was resected or preserved, the patients were divided into the ACDF with UT group (n = 37) and the ACDF without UT group (n = 50). Perioperative data, radiographic parameters, clinical outcomes, and complications were compared between the two groups.
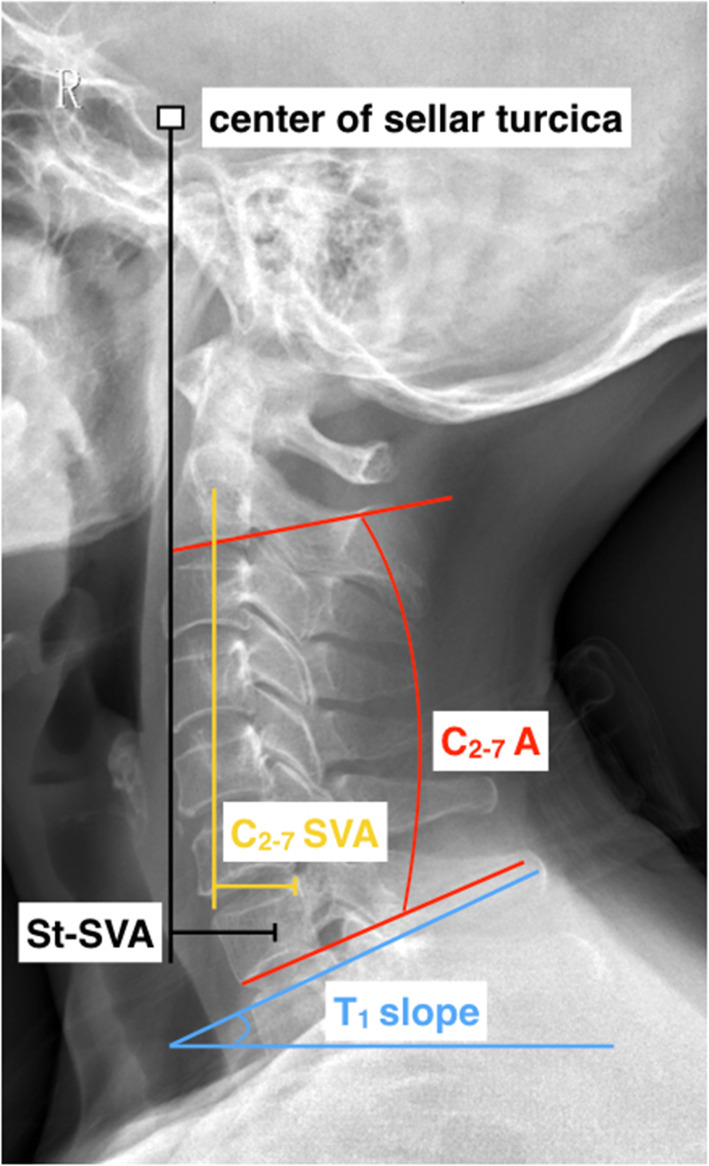
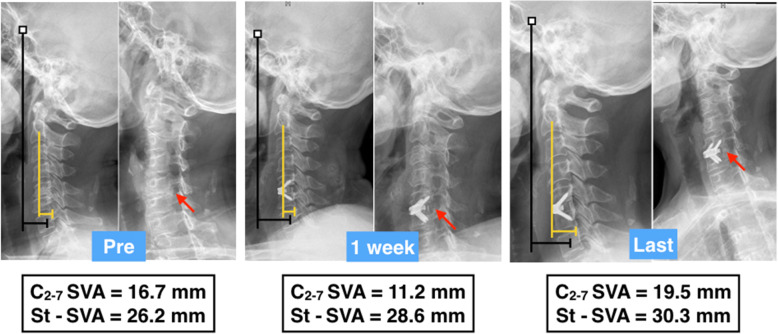
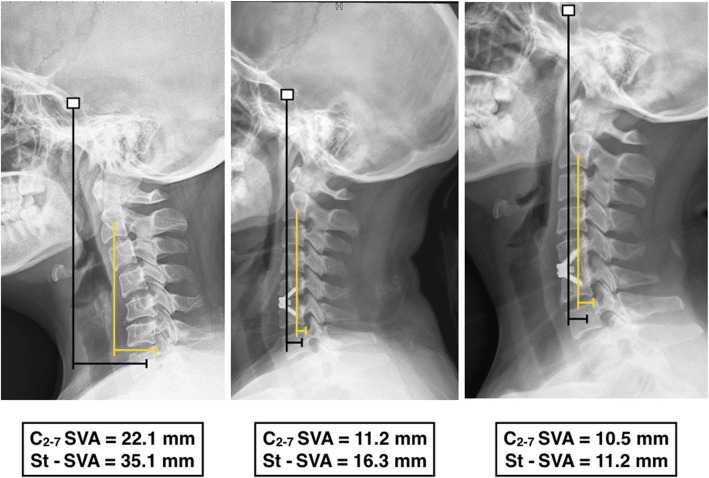
Results: The mean follow-up was 16.86 ± 5.63 and 18.36 ± 7.51 months in the ACDF with UT group and ACDF without UT group, respectively (p > 0.05). The average preoperative VAS arm score was 5.89 ± 1.00 in the ACDF with UT group and 5.18 ± 1.21 in the ACDF without UT group (p = 0.038). However, the average VAS arm score was 4.22 ± 0.64, 4.06 ± 1.13 and 1.68 ± 0.71, 1.60 ± 0.70 at 1 week post operation and at final follow up, respectively, (p > 0.05). We also found that the C2-7 SVA and St-SVA at the last follow-up and their change (last follow-up value - preoperative value) in the ACDF with UT group were significantly higher than ACDF without UT group (p < 0.05). No marked differences in the other cervical sagittal parameters, fusion rate or complications, including dysphagia, ASD, and subsidence, were observed.
Conclusions: Our result indicates that ACDF using a zero-p implant with or without partial UT both provide satisfactory clinical efficacy and acceptable safety. However, additional partial UT may has a negative effect on cervical sagittal alignment.
Keywords: Anterior cervical discectomy and fusion; Cervical spondylotic radiculopathy; Incinatectomy; Sagittal alignment; Uncovertebral joint.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
