

Cognitive Impairment After Intracerebral Hemorrhage: A Systematic Review of Current Evidence and Knowledge Gaps
- PMID: 34512528
- PMCID: PMC8429504
- DOI: 10.3389/fneur.2021.716632
Cognitive Impairment After Intracerebral Hemorrhage: A Systematic Review of Current Evidence and Knowledge Gaps
Abstract
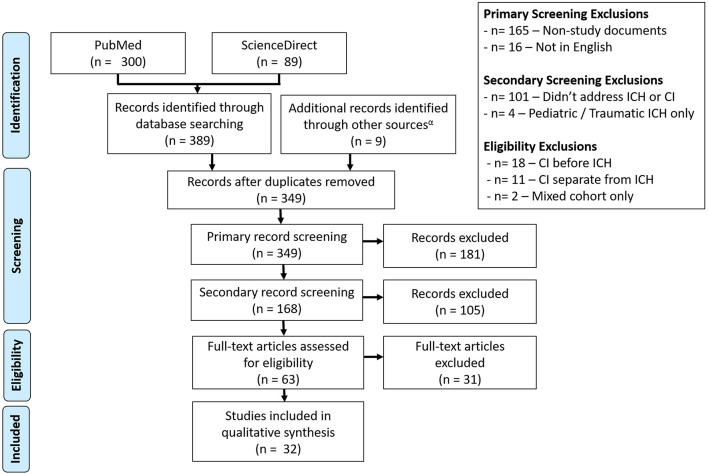
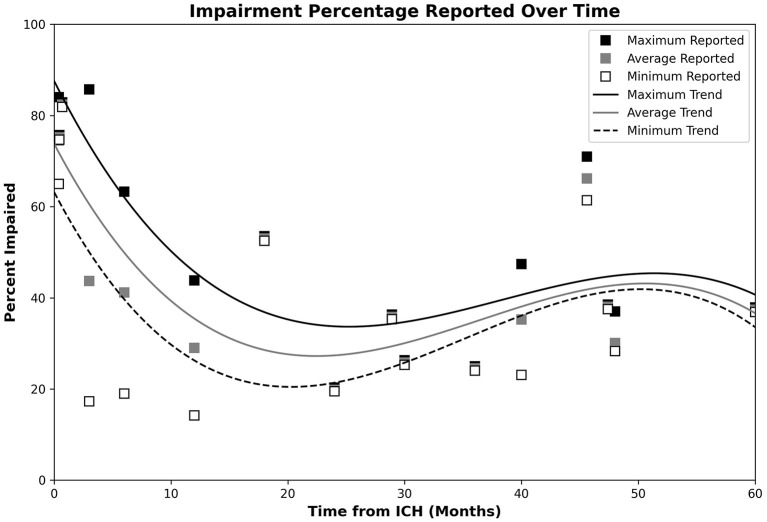
Background: Cognitive impairment (CI) is commonly observed after intracerebral hemorrhage (ICH). While a growing number of studies have explored this association, several evidence gaps persist. This review seeks to investigate the relationship between CI and ICH. Methods: A two-stage systematic review of research articles, clinical trials, and case series was performed. Initial search used the keywords ["Intracerebral hemorrhage" OR "ICH"] AND ["Cognitive Impairment" OR "Dementia OR "Cognitive Decline"] within the PubMed (last accessed November 3rd, 2020) and ScienceDirect (last accessed October 27th, 2020) databases, without publication date limits. Articles that addressed CI and spontaneous ICH were accepted if CI was assessed after ICH. Articles were rejected if they did not independently address an adult human population or spontaneous ICH, didn't link CI to ICH, were an unrelated document type, or were not written in English. A secondary snowball literature search was performed using reviews identified by the initial search. The Agency for Healthcare research and Quality's assessment tool was used to evaluate bias within studies. Rates of CI and contributory factors were investigated. Results: Search yielded 32 articles that collectively included 22,631 patients. Present evidence indicates a high rate of post-ICH CI (65-84%) in the acute phase (<4 weeks) which is relatively lower at 3 (17.3-40.2%) and 6 months (19-63.3%). Longer term follow-up (≥1 year) demonstrates a gradual increase in CI. Advanced age, female sex, and prior stroke were associated with higher rates of CI. Associations between post-ICH CI and cerebral microbleeds, superficial siderosis, and ICH volume also exist. Pre-ICH cognitive assessment was missing in 28% of included studies. The Mini Mental State Evaluation (44%) and Montreal Cognitive Assessment (16%) were the most common cognitive assessments, albeit with variable thresholds and definitions. Studies rarely (<10%) addressed racial and ethnic disparities. Discussion: Current findings suggest a dynamic course of post-ICH cognitive impairment that may depend on genetic, sociodemographic and clinical factors. Methodological heterogeneity prevented meta-analysis, limiting results. There is a need for the methodologies and time points of post-ICH cognitive assessments to be harmonized across diverse clinical and demographic populations.
Keywords: cerebral small vessel disease; cognitive impairment; dementia; intracerebral hemorrhage; outcome; stroke.
Copyright © 2021 Potter, Lioutas, Tano, Pan, Meeks, Woo, Seshadri, Selim and Vahidy.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources