

Dialyzer Classification and Mortality in Hemodialysis Patients: A 3-Year Nationwide Cohort Study
- PMID: 34513892
- PMCID: PMC8429602
- DOI: 10.3389/fmed.2021.740461
Dialyzer Classification and Mortality in Hemodialysis Patients: A 3-Year Nationwide Cohort Study
Abstract
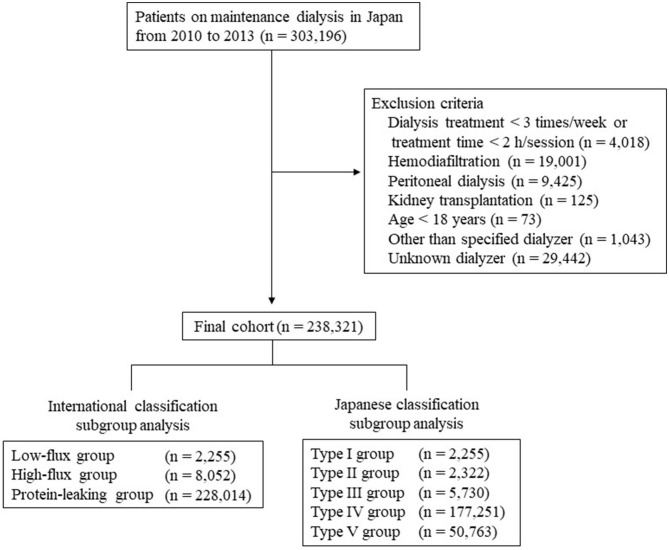
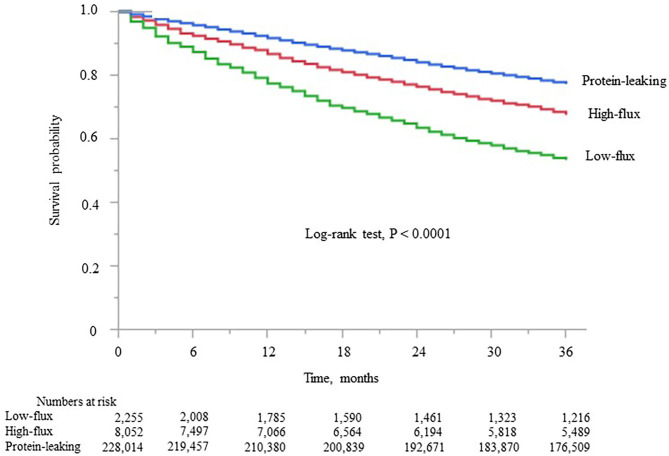
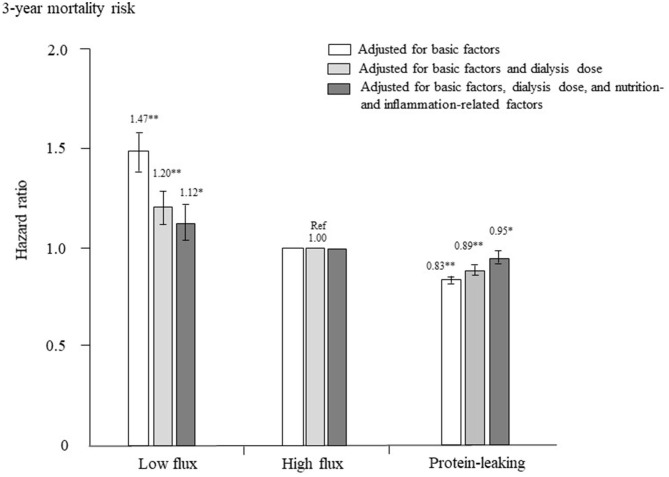
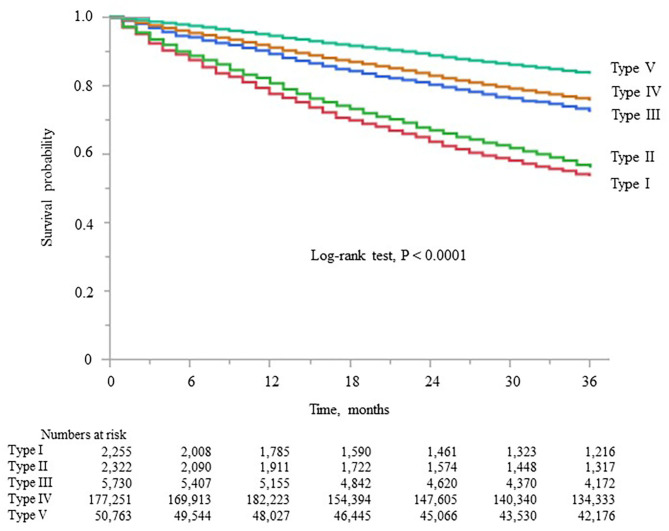
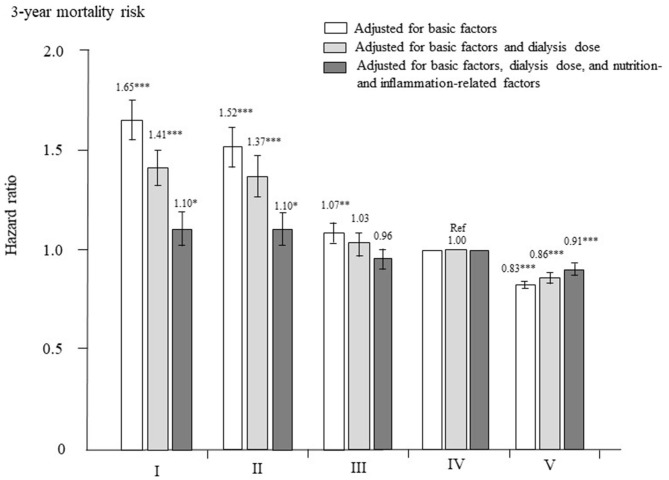
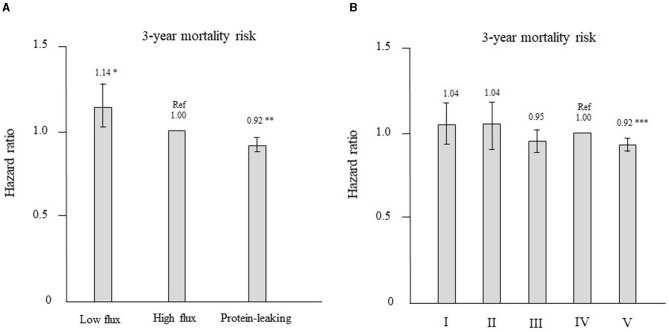
Background: Dialyzers are classified as low-flux, high-flux, and protein-leaking membrane dialyzers internationally and as types I, II, III, IV, and V based on β2-microglobulin clearance rate in Japan. Type I dialyzers correspond to low-flux membrane dialyzers, types II and III to high-flux membrane dialyzers, and types IV and V to protein-leaking membrane dialyzers. Here we aimed to clarify the association of dialyzer type with mortality. Methods: This nationwide retrospective cohort study analyzed data from the Japanese Society for Dialysis Therapy Renal Data Registry from 2010 to 2013. We enrolled 238,321 patients on hemodialysis who were divided into low-flux, high-flux, and protein-leaking groups in the international classification and into type I to V groups in the Japanese classification. We assessed the associations of each group with 3-year all-cause mortality using Cox proportional hazards models and performed propensity score matching analysis. Results: By the end of 2013, 55,308 prevalent dialysis patients (23.2%) had died. In the international classification subgroup analysis, the hazard ratio (95% confidence interval) was significantly higher in the low-flux group [1.12 (1.03-1.22), P = 0.009] and significantly lower in the protein-leaking group [0.95 (0.92-0.98), P = 0.006] compared with the high-flux group after adjustment for all confounders. In the Japanese classification subgroup analysis, the hazard ratios were significantly higher for types I [1.10 (1.02-1.19), P = 0.015] and II [1.10 (1.02-1.39), P = 0.014] but significantly lower for type V [0.91 (0.88-0.94), P < 0.0001] compared with type IV after adjustment for all confounders. These significant findings persisted after propensity score matching under both classifications. Conclusions: Hemodialysis using protein-leaking dialyzers might reduce mortality rates. Furthermore, type V dialyzers are superior to type IV dialyzers in hemodialysis patients.
Keywords: hemodialysis; high-flux dialyzer; low-flux dialyzer; mortality; protein-leaking dialyzer; β2-microglobulin clearance.
Copyright © 2021 Abe, Masakane, Wada, Nakai, Nitta and Nakamoto.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Brown PH, Kalra PA, Turney JH, Cooper EH. Serum low-molecular-weight proteins in haemodialysis patients: effect of residual renal function. Nephrol Dial Transplant. (1988) 3:169–73. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials