

Conventional oxygen therapy versus CPAP as a ceiling of care in ward-based patients with COVID-19: a multi-centre cohort evaluation
- PMID: 34514360
- PMCID: PMC8424135
- DOI: 10.1016/j.eclinm.2021.101122
Conventional oxygen therapy versus CPAP as a ceiling of care in ward-based patients with COVID-19: a multi-centre cohort evaluation
Abstract
Background: Continuous positive airway pressure (CPAP) therapy is commonly used for respiratory failure due to severe COVID-19 pneumonitis, including in patients deemed not likely to benefit from invasive mechanical ventilation (nIMV). Little evidence exists demonstrating superiority over conventional oxygen therapy, whilst ward-level delivery of CPAP presents practical challenges. We sought to compare clinical outcomes of oxygen therapy versus CPAP therapy in patients with COVID-19 who were nIMV.
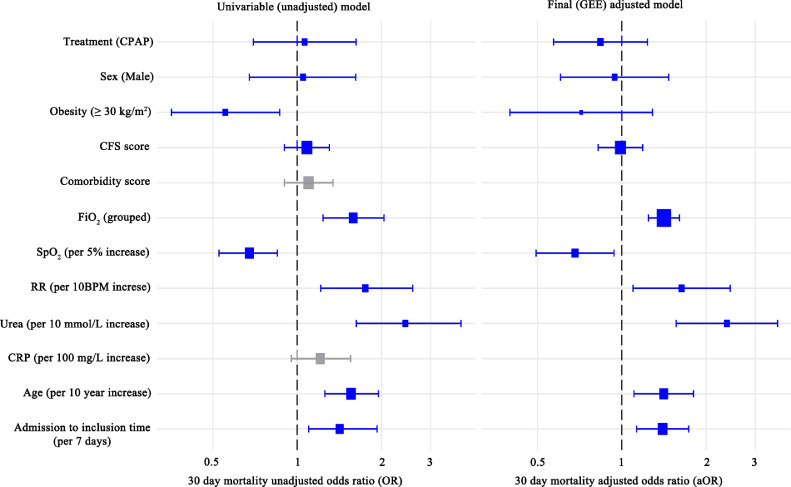
Methods: This retrospective multi-centre cohort evaluation included patients diagnosed with COVID-19 who were nIMV, had a treatment escalation plan of ward-level care and clinical frailty scale ≤ 6. Recruitment occurred during the first two waves of the UK COVID-19 pandemic in 2020; from 1st March to May 31st, and from 1st September to 31st December. Patients given CPAP were compared to patients receiving oxygen therapy that required FiO2 ≥0.4 for more than 12 hours at hospitals not providing ward-level CPAP. Logistic regression modelling was performed to compare 30-day mortality between treatment groups, accounting for important confounders and within-hospital clustering.
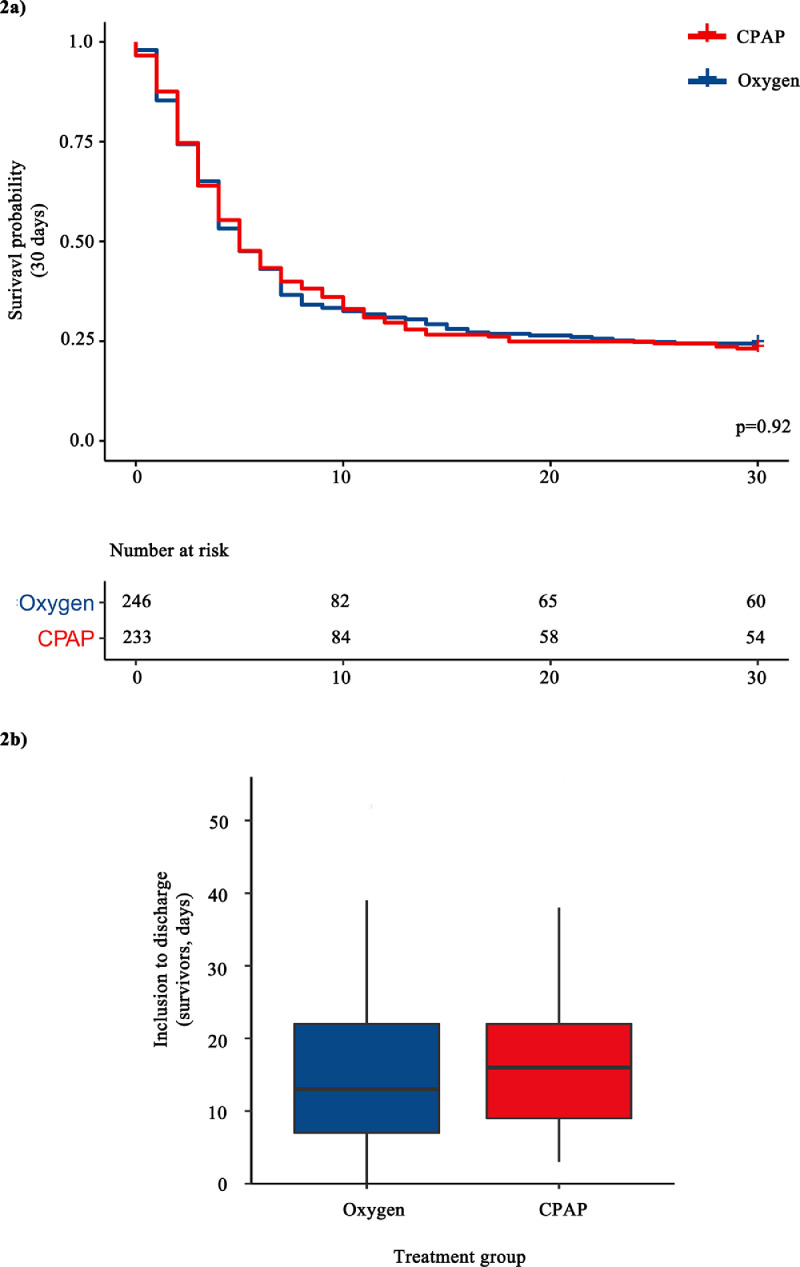
Findings: Seven hospitals provided data for 479 patients during the UK COVID-19 pandemic in 2020. Overall 30-day mortality was 75.6% in the oxygen group (186/246 patients) and 77.7% in the CPAP group (181/233 patients). A lack of evidence for a treatment effect persisted in the adjusted model (adjusted odds ratio 0.84 95% CI 0.57-1.23, p=0.37). 49.8% of patients receiving CPAP-therapy (118/237) chose to discontinue it.
Interpretation: No survival difference was found between using oxygen alone or CPAP to treat patients with severe COVID-19 who were nIMV. A high patient-initiated discontinuation rate for CPAP suggests a significant treatment burden. Further reflection is warranted on the current treatment guidance and widespread application of CPAP in this setting.
Funding: L Pearmain is supported by the MRC (MR/R00191X/1). TW Felton is supported by the NIHR Manchester Biomedical Research Centre.
Keywords: COVID-19; Ceiling of care; Invasive mechanical ventilation; Non-invasive ventilation; Oxygen; nIMV.
© 2021 The Authors.
Conflict of interest statement
AB reports fees for speaking/session chair for Fisher and Paykel webinars (high nasal flow cannulae). AB is an advisory board member for Sanofi Genzyme (respiratory management of Pompe disease). All other authors have nothing to declare.
Figures
References
-
- Scottish Intercollegiate Guidelines Network (SIGN). COVID-19 position statement: CPAP for COVID-19 related respiratory failure [Internet]. 2020 [updated 2020 Sept, cited 2021 July]. Available from http://www.sign.ac.uk.
-
- NHS England and NHS Improvement. Guidance for the role and use of non-invasive respiratory support in adult patients with coronavirus (confirmed or suspected) [Discontinued] [Internet]. 2020 [updated 2020 Apr, cited 2021 Jul]. Available from: https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/....
-
- World Health Organisation (WHO). Clinical management of severe acute respiratory infection (SARI) when COVID-19 disease is suspected: interim guidance [Internet]. 2019 [updated 2020 Mar, cited 2021 Jul]. Available from: https://apps.who.int/iris/handle/10665/331446.
Grants and funding
LinkOut - more resources
Full Text Sources
