

Gastrointestinal tolerability of once-weekly semaglutide 2.4 mg in adults with overweight or obesity, and the relationship between gastrointestinal adverse events and weight loss
- PMID: 34514682
- PMCID: PMC9293236
- DOI: 10.1111/dom.14551
Gastrointestinal tolerability of once-weekly semaglutide 2.4 mg in adults with overweight or obesity, and the relationship between gastrointestinal adverse events and weight loss
Abstract
Aim: We evaluated gastrointestinal (GI) adverse events (AEs) with once-weekly semaglutide 2.4 mg in adults with overweight or obesity and their contribution to weight loss (WL).
Materials and methods: AE analyses pooled data from the Semaglutide Treatment Effect in People With Obesity (STEP) 1-3 trials for participants randomized to 68 weeks of semaglutide 2.4 mg (n = 2117) or placebo (n = 1262). WL was analysed by presence/absence of GI AEs. Mediation analysis estimated WL effects mediated by and unrelated to GI AEs. GI tolerability with semaglutide 2.4 mg maintenance and cessation after dose escalation was evaluated using STEP 4 data among 803 participants tolerating 20 weeks of semaglutide run-in.
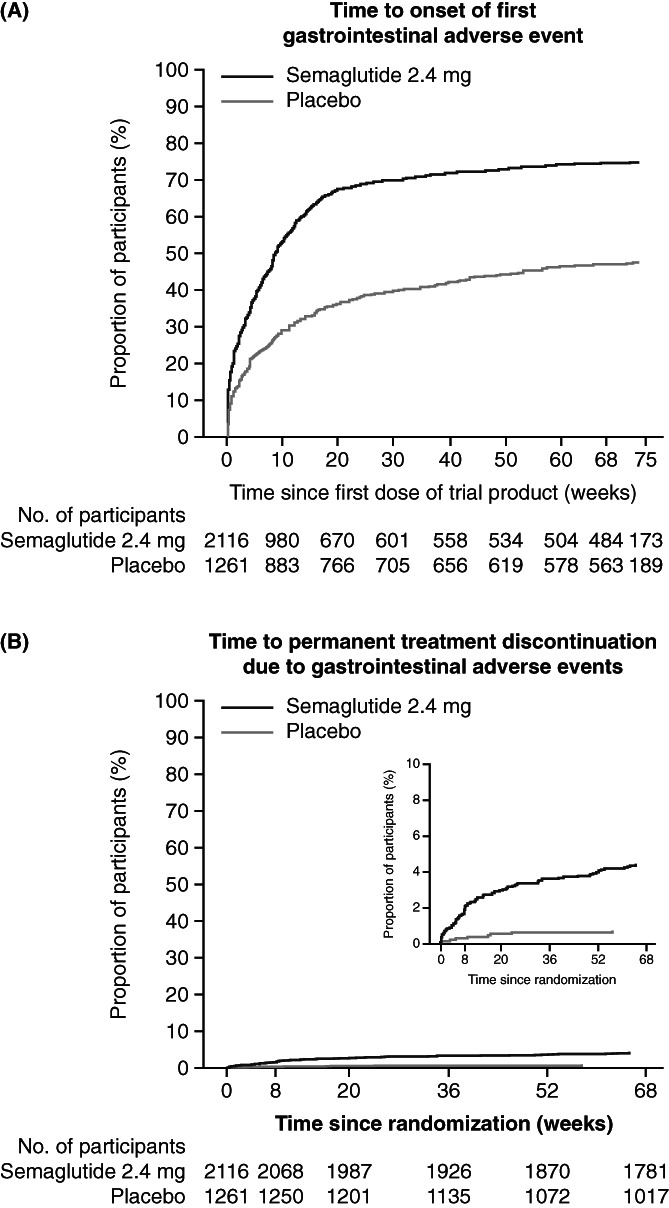
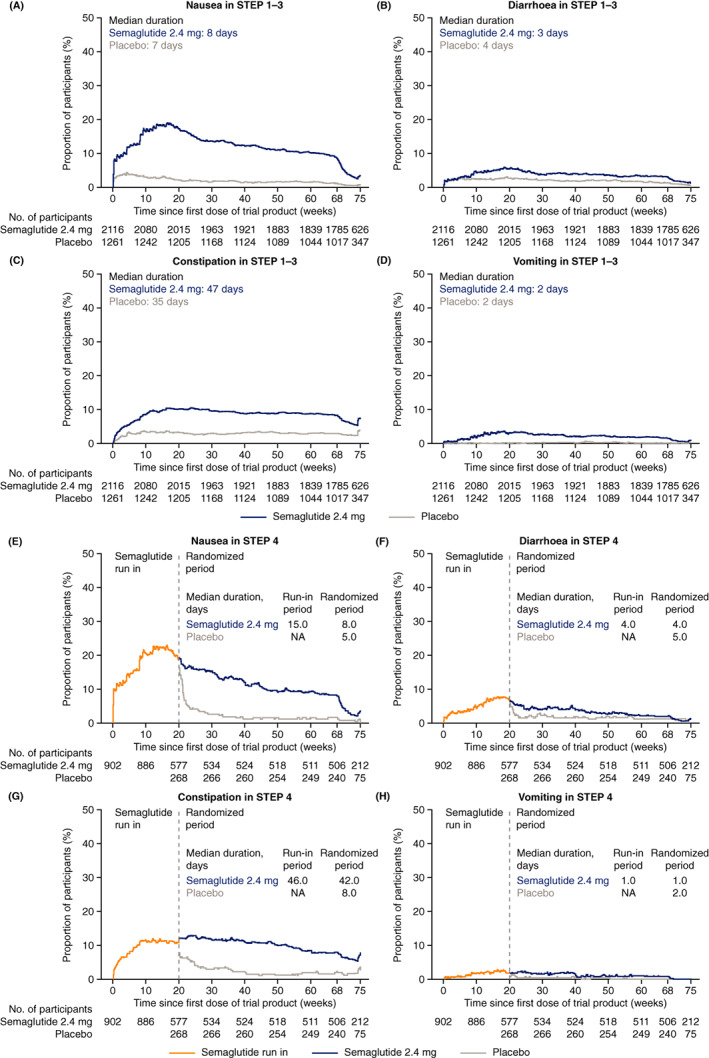
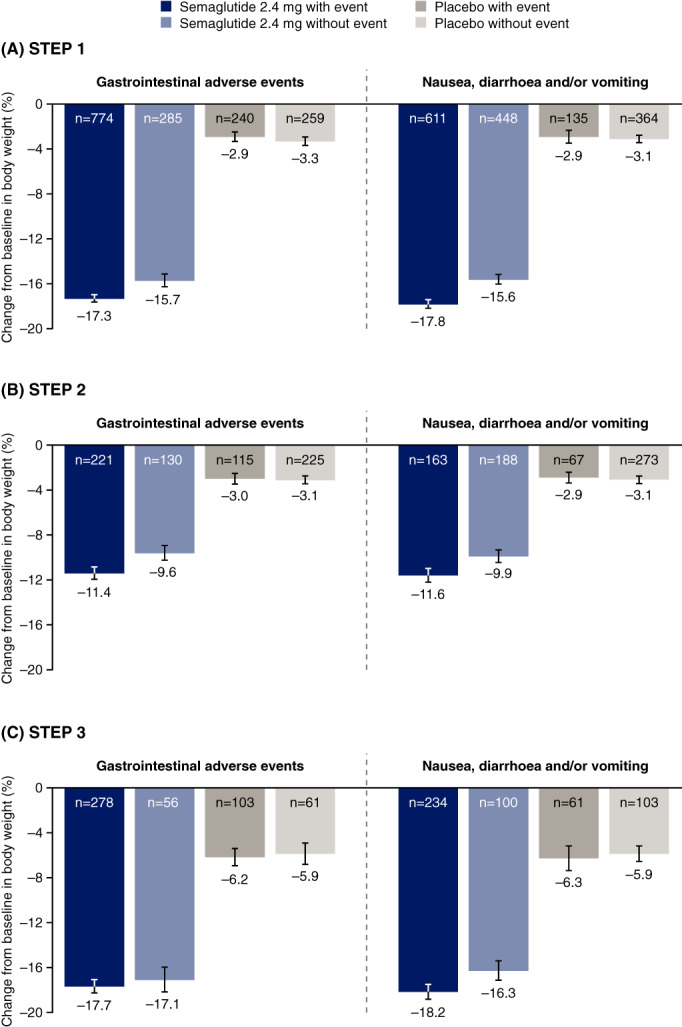
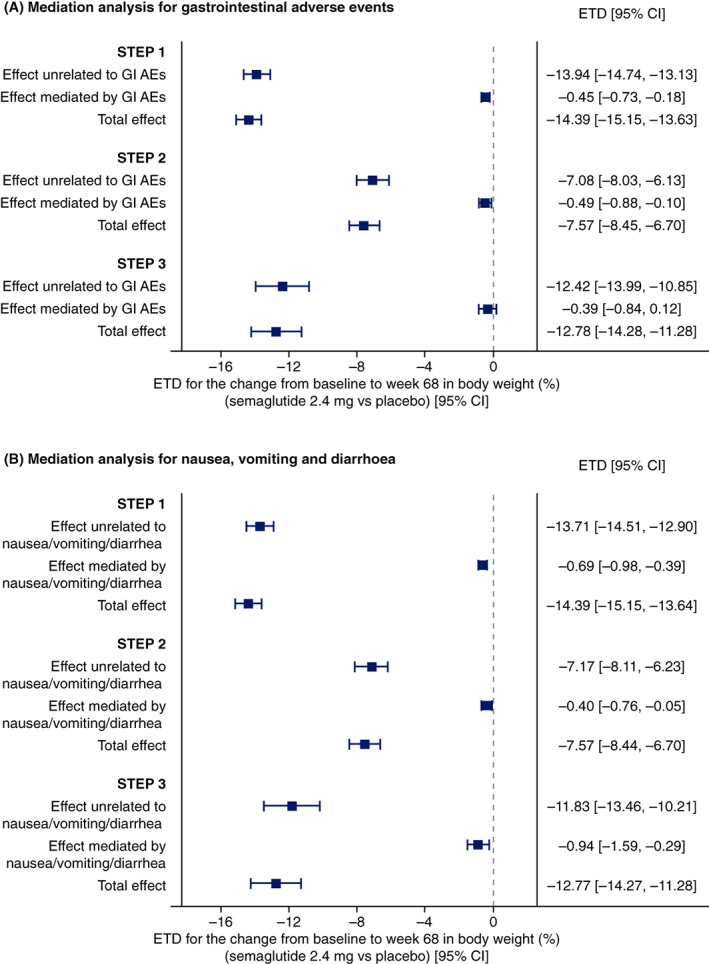
Results: GI AEs were more common with semaglutide 2.4 mg than placebo, with most frequently nausea (43.9% vs. 16.1% of participants), diarrhoea (29.7% vs. 15.9%), vomiting (24.5% vs. 6.3%) and constipation (24.2% vs. 11.1%). Most GI AEs with semaglutide were non-serious (99.5% of AEs), mild-to-moderate (98.1%), transient and occurred most frequently during/shortly after dose escalation. Few semaglutide-treated participants (4.3%) permanently discontinued treatment for GI AEs. In STEP 1-3, mean WL with semaglutide 2.4 mg was similar in participants without (9.6%-17.1%) versus with GI AEs (11.4%-17.7%). Consistent with this observation, mediation analysis found that GI AEs contributed little to semaglutide-induced WL: of the additional 7.6%-14.4% WL with semaglutide versus placebo, <1 percentage point was mediated by GI AEs. In STEP 4, semaglutide 2.4 mg maintenance was well tolerated.
Conclusions: GI AEs were more common with semaglutide 2.4 mg than placebo, but typically mild-to-moderate and transient. Semaglutide-induced WL was largely independent of GI AEs.
Keywords: GLP-1 analogue; antiobesity drug; obesity therapy; phase III study; randomized trial; weight control.
© 2021 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
SW reports research funding, advisory/consulting fees and/or other support from AstraZeneca, Bausch Health Inc., Boehringer Ingelheim, CIHR, Janssen, Lilly and Novo Nordisk. SC is an employee of and shareholder at Novo Nordisk A/S. MD is a consultant, advisory board member and speaker for AstraZeneca, Boehringer Ingelheim, Janssen, Lilly, Merck Sharp & Dohme, Novo Nordisk and Sanofi‐Aventis; advisory board member for Gilead Sciences Ltd. and Servier; speaker for Mitsubishi Tanabe Pharma Corporation, NAPP and Takeda Pharmaceuticals International Inc.; received research funding from AstraZeneca, Boehringer Ingelheim, Janssen, Lilly, Novo Nordisk and Sanofi‐Aventis. MD is also co‐funded by the NIHR Leicester Biomedical Research Centre. DD is a consultant, advisory board member and speaker for AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Novo Nordisk and Sanofi‐Aventis; received research funding from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Novo Nordisk and Sanofi‐Aventis. BG is an employee of and shareholder at Novo Nordisk A/S. IL reports research funding, advisory/consulting fees and/or other support from AstraZeneca, Bayer, Boehringer Ingelheim, Eli Lilly, GI Dynamics, Intarcia, Intercept, Janssen, Mannkind, Merck, Mylan, Novartis, Novo Nordisk, Pfizer, Sanofi, TARGETPharma, Valeritas and Zealand Pharma. OM is an advisory board member for AstraZeneca, Boehringer Ingelheim, BOL Pharma, Eli Lilly, Merck Sharp & Dohme, Novo Nordisk and Sanofi; received research grant support through Hadassah Hebrew University Hospital from AstraZeneca and Novo Nordisk; speaker's bureau for AstraZeneca, Boehringer Ingelheim, Eli Lilly, Janssen, Merck Sharp & Dohme, Novo Nordisk and Sanofi. DMR is a consultant, advisory board member, speaker and clinical investigator for Novo Nordisk; clinical investigator for AstraZeneca and Boehringer Ingelheim; received honoraria from Medscape; received research funding from Obesinov and SARL; holds stock/shares in Novo Nordisk. MT is an employee of and shareholder at Novo Nordisk A/S. TAW serves on advisory boards for Novo Nordisk and WW (formerly Weight Watchers) and has received grant support, on behalf of the University of Pennsylvania, from Novo Nordisk. SDP has received consulting fees and/or speaking honoraria from Abbott, AstraZeneca, Bausch, Bayer, Boehringer Ingelheim, Dexcom, Eli Lilly, HLS, Janssen, Merck, Novo Nordisk and Sanofi; was involved in research studies for Abbott, AstraZeneca, Bausch, Boehringer Ingelheim, Eli Lilly, Janssen, Merck, Novo Nordisk and Sanofi.
Figures
References
-
- Garvey WT, Mechanick JI, Brett EM, et al. American Association of Clinical Endocrinologists and American College of Endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocr Pract. 2016;22(suppl 3):1‐203. 10.4158/EP161365.GL - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
