

LVS-HARMED Risk Score for Incident Heart Failure in Patients With Atrial Fibrillation Who Present to the Emergency Department: Data from a World-Wide Registry
- PMID: 34514842
- PMCID: PMC8649506
- DOI: 10.1161/JAHA.120.017735
LVS-HARMED Risk Score for Incident Heart Failure in Patients With Atrial Fibrillation Who Present to the Emergency Department: Data from a World-Wide Registry
Abstract
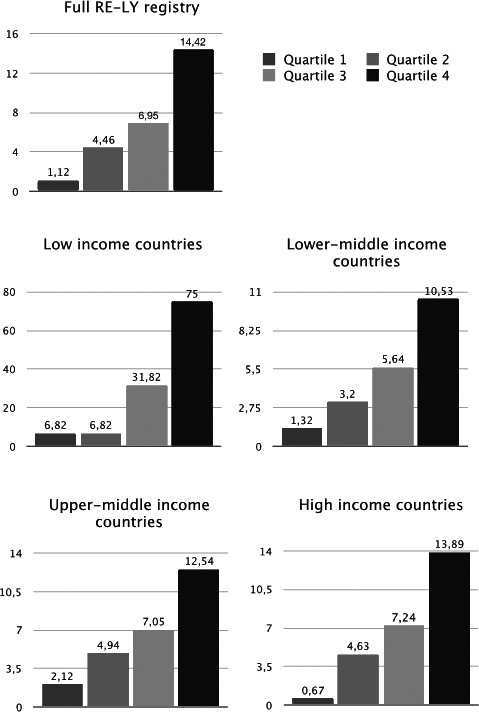
Background Heart failure (HF) is a common complication to atrial fibrillation (AF), leading to rehospitalization and death. Early identification of patients with AF at risk for HF might improve outcomes. We aimed to derive a score to predict 1-year risk of new-onset HF after an emergency department (ED) visit with AF. Methods and Results The RE-LY AF (Randomized Evaluation of Long-Term Anticoagulant Therapy) registry enrolled patients with AF presenting to an ED in 47 countries, and followed them for a year. The end point was HF hospitalization and/or HF death. Among 15 400 ED patients, 9765 had no prior HF (mean age, 64.9±14.9 years). Within 1 year, new-onset HF developed in 6.8% of patients, of whom 21% died of HF. Independent predictors of HF included left ventricular hypertrophy (odds ratio [OR], 1.47; 95% CI, 1.19-1.82), valvular heart disease (OR, 1.55; 95% CI, 1.18-2.04), smoking (OR, 1.42; 95% CI, 1.12-1.78), height (OR, 0.93; 95% CI, 0.90-0.95 per 3 cm), age (OR, 1.11; 95% CI, 1.07-1.15 per 5 years), rheumatic heart disease (OR, 1.77, 95% CI, 1.24-2.51), prior myocardial infarction (OR, 1.85; 95% CI, 1.45-2.36), remaining in AF at ED discharge (OR, 1.86; 95% CI, 1.46-2.36), and diabetes (OR, 1.33; 95% CI, 1.09-1.64). A continuous risk prediction score (LVS-HARMED [left ventricular, valvular heart disease, smoking or other tobacco use, height, age, rheumatic heart disease, myocardial infarction, emergency department discharge rhythm, and diabetes]) had good discrimination (C statistic, 0.735; 95% CI, 0.716-0.755). Validation was conducted internally using bootstrapping (optimism-corrected C statistic, 0.705) and externally (C statistic, 0.699). The 1-year incidence of HF hospitalization and/or HF death across quartile groups of the score was 1.1%, 4.5%, 6.9%, and 14.4%, respectively. LVS-HARMED also predicted incident stroke (C statistic, 0.753; 95% CI, 0.728-0.778). Conclusions The LVS-HARMED score predicts new-onset HF after an ED visit for AF. Preventative strategies should be considered in patients with high LVS-HARMED HF risk.
Keywords: atrial fibrillation; epidemiology; heart failure; prevention; risk score; risk stratification.
Conflict of interest statement
None.
Figures
References
-
- Healey JS, Oldgren J, Ezekowitz M, Zhu J, Pais P, Wang J, Commerford P, Jansky P, Avezum A, Sigamani A, et al.; Registry R‐LAF and Cohort Study I . Occurrence of death and stroke in patients in 47 countries 1 year after presenting with atrial fibrillation: a cohort study. Lancet. 2016;388:1161–1169. DOI: 10.1016/S0140-6736(16)30968-0. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
