

Clinical, Pathological, and Prognostic Analysis of Urachal Carcinoma
- PMID: 34515250
- PMCID: PMC8985044
- DOI: 10.1159/000518028
Clinical, Pathological, and Prognostic Analysis of Urachal Carcinoma
Abstract
Objective: The aim of this study was to improve understanding the clinical, pathologic, and prognostic features of urachal carcinoma (UrC), a retrospectively descriptive study was done in 2 clinical centers.
Methods: After excluding the 2 missed patients, the clinical and pathological data of 59 patients with UrC, who were diagnosed or treated at 2 clinical centers between 1986 and 2019, was retrospectively analyzed. SPSS 22.0 (IBM) and GraphPad Prism 8.0.1 were used for statistics and data visualization. Survival data were analyzed by the Kaplan-Meier method and Log-rank tests. Cox proportional hazards regression were performed for find risk factors on predicting the prognosis.
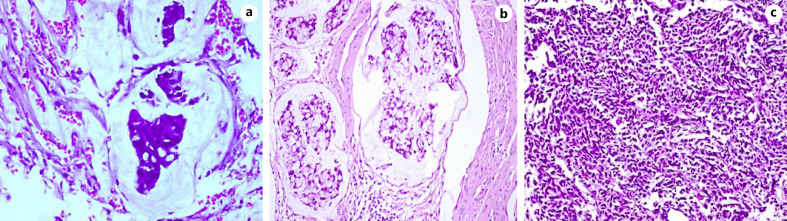
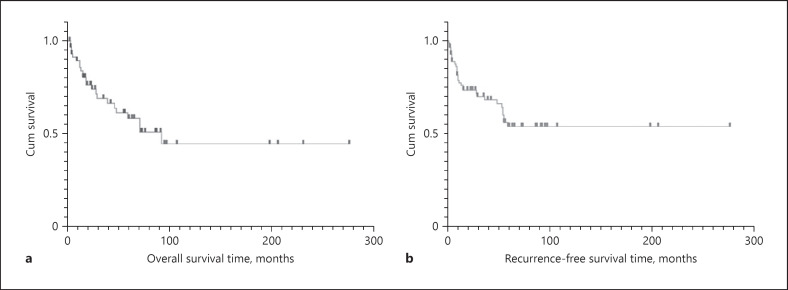
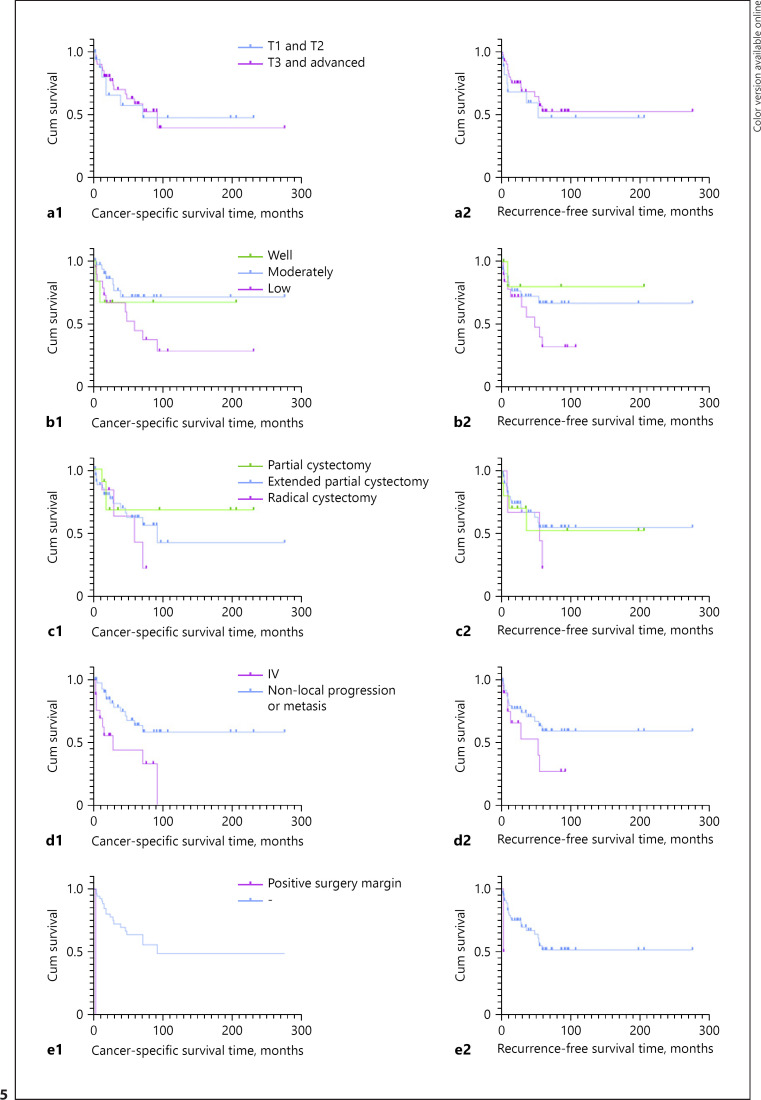
Results: Of all 59 patients, 47 were male and 12 were female. The median age at diagnosis was 51.6 years (range: 22-84 years). Gross hematuria was the most common symptom (79.66%). The majority of urachal neoplasms were adenocarcinomas (94.92%). Forty-two patients (72.41%) underwent extended partial cystectomy with en bloc resection of the entire urachus. The mean follow-up was 52 months (3-277 months). Median overall survival was 52.8 months (4-93 months). The 3-year cancer-specific survival (CSS) rate and 5-year CSS rate were 69.1% and 61.2%. There was no significant difference among localized T stage, tumor histologic grade and surgical procedures in determining prognosis by survival analyze. While patients with high-risk TNM stage (local abdominal metastasis, lymph node metastasis, or distant metastasis) (p = 0.003) and positive surgical margin (p < 0.001) had significantly worse prognosis.
Conclusions: The results indicate that high-risk TNM stage and positive surgical margin are risk predictors of prognosis. Localized T stage, histologic grade, and surgical procedure cause no significant effect on patient prognosis. The extended partial cystectomy is the recommended surgical approach for patients with UrC. Active multimodal treatments may improve the survival of patients with recurrent and metastatic disease.
Keywords: Adjuvant therapy; Extended partial cystectomy; High-risk TNM stage; Positive surgical margin; Prognosis; Urachal carcinoma.
© 2021 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Frimberger DC, Kropp BP. Bladder anomalies in children. Campbell-Walsh Urol. 2012:3379–88.
-
- Paras FA, MacLennan GT. Urachal adenocarcinoma. J Urol. 2008;180((2)):720–0. - PubMed
-
- Wright JL, Porter MP, Li CI, Lange PH, Lin DW. Differences in survival among patients with urachal and nonurachal adenocarcinomas of the bladder. Cancer. 2006 Aug 15;107((4)):721–8. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
