

Capecitabine Versus Active Monitoring in Stable or Responding Metastatic Colorectal Cancer After 16 Weeks of First-Line Therapy: Results of the Randomized FOCUS4-N Trial
- PMID: 34516759
- PMCID: PMC8601309
- DOI: 10.1200/JCO.21.01436
Capecitabine Versus Active Monitoring in Stable or Responding Metastatic Colorectal Cancer After 16 Weeks of First-Line Therapy: Results of the Randomized FOCUS4-N Trial
Abstract
Purpose: Despite extensive randomized evidence supporting the use of treatment breaks in metastatic colorectal cancer (mCRC), they are not universally offered to patients despite improvements in quality of life without detriment to overall survival (OS). FOCUS4-N was set up to explore the impact of oral maintenance therapy in patients who are responding to first-line therapy.
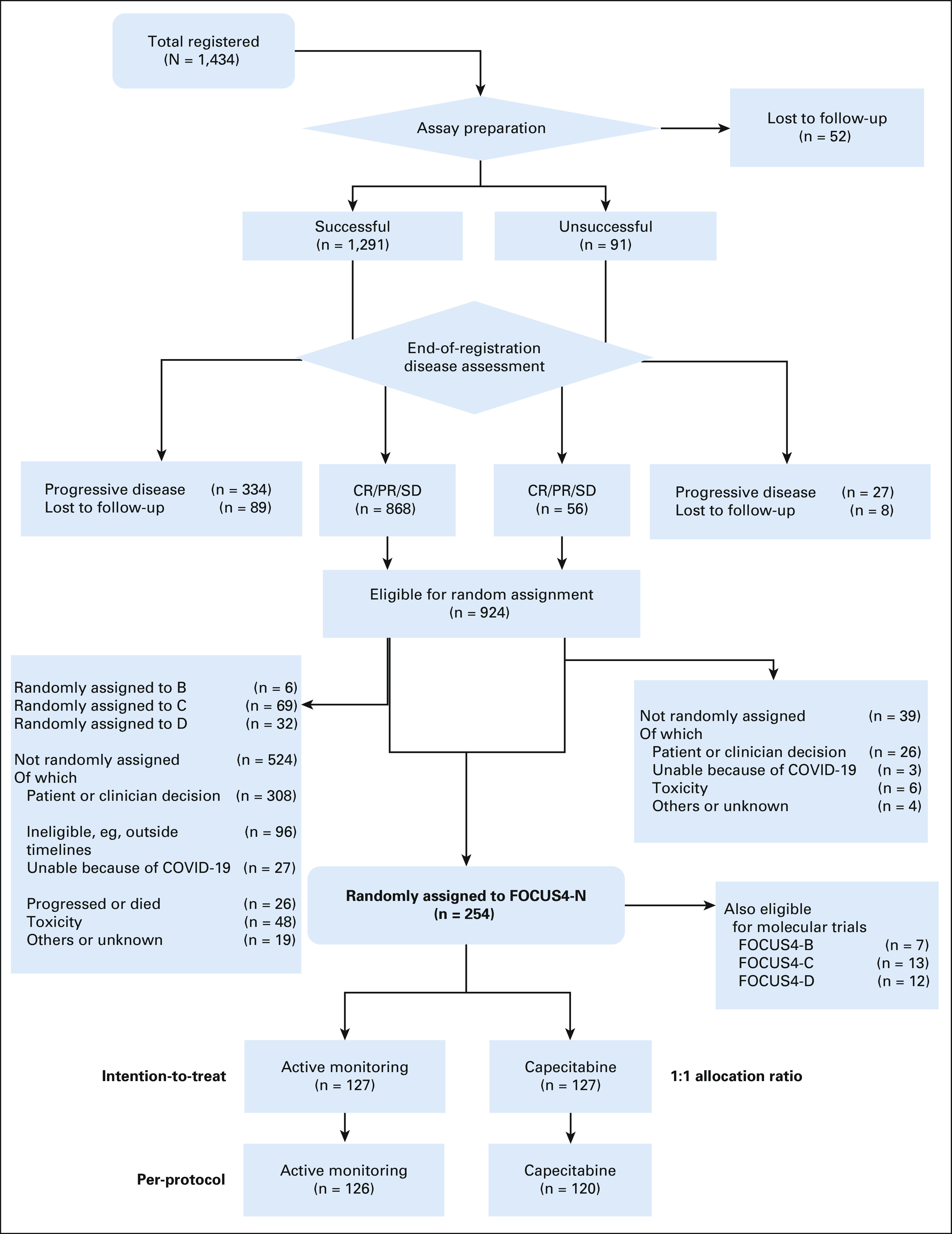
Methods: FOCUS4 was a molecularly stratified trial program that registered patients with newly diagnosed mCRC. The FOCUS4-N trial was offered to patients in whom a targeted subtrial was unavailable or biomarker tests failed. Patients were randomly assigned using a 1:1 ratio between maintenance capecitabine and active monitoring (AM). The primary outcome was progression-free survival (PFS) with secondary outcomes including OS toxicity and tolerability.
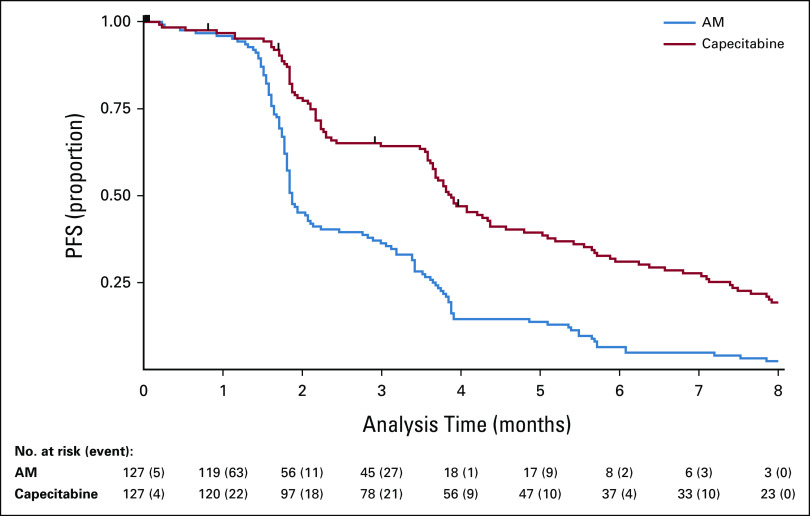
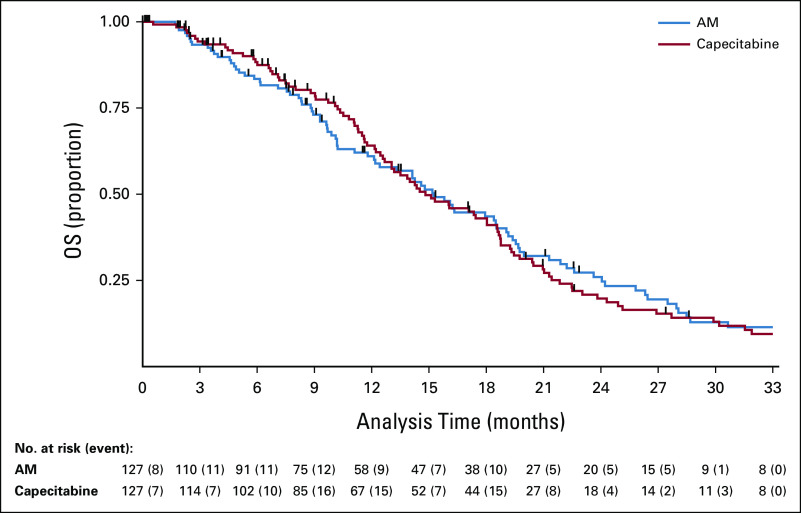
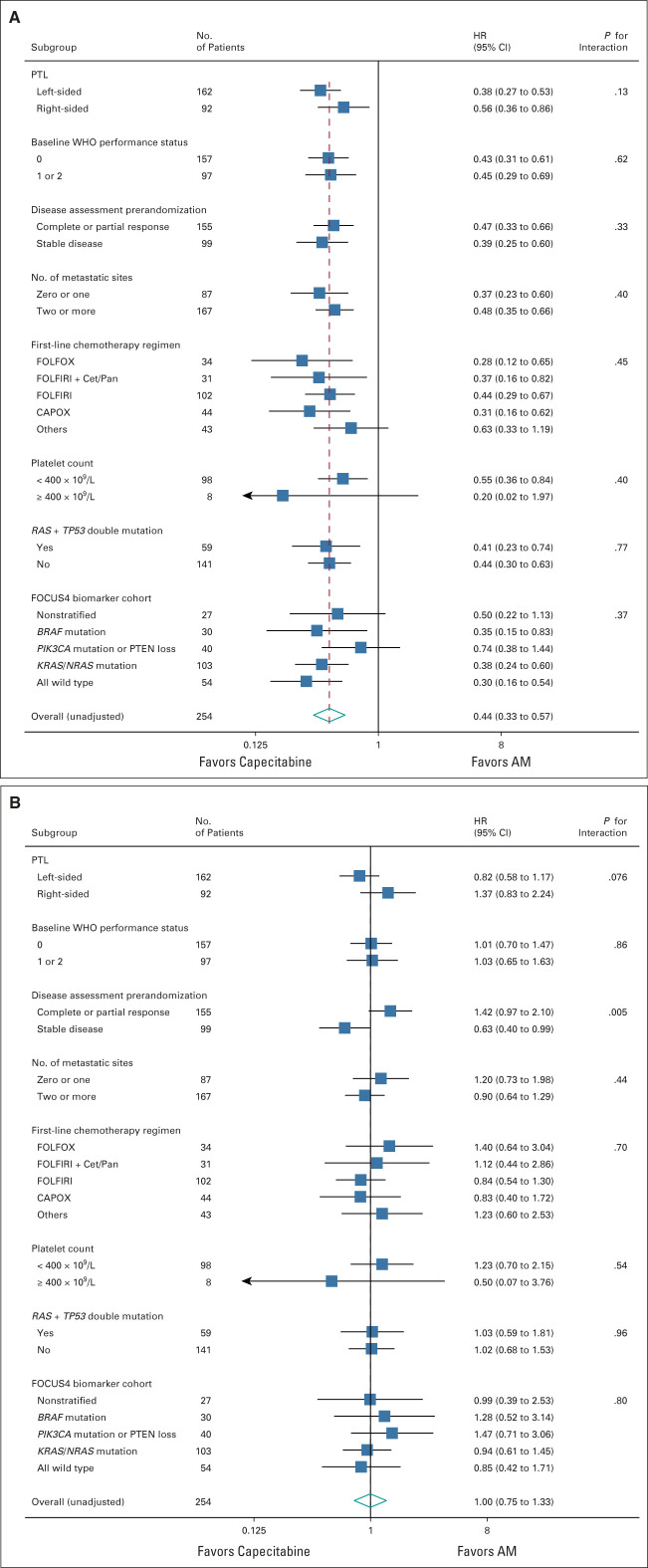
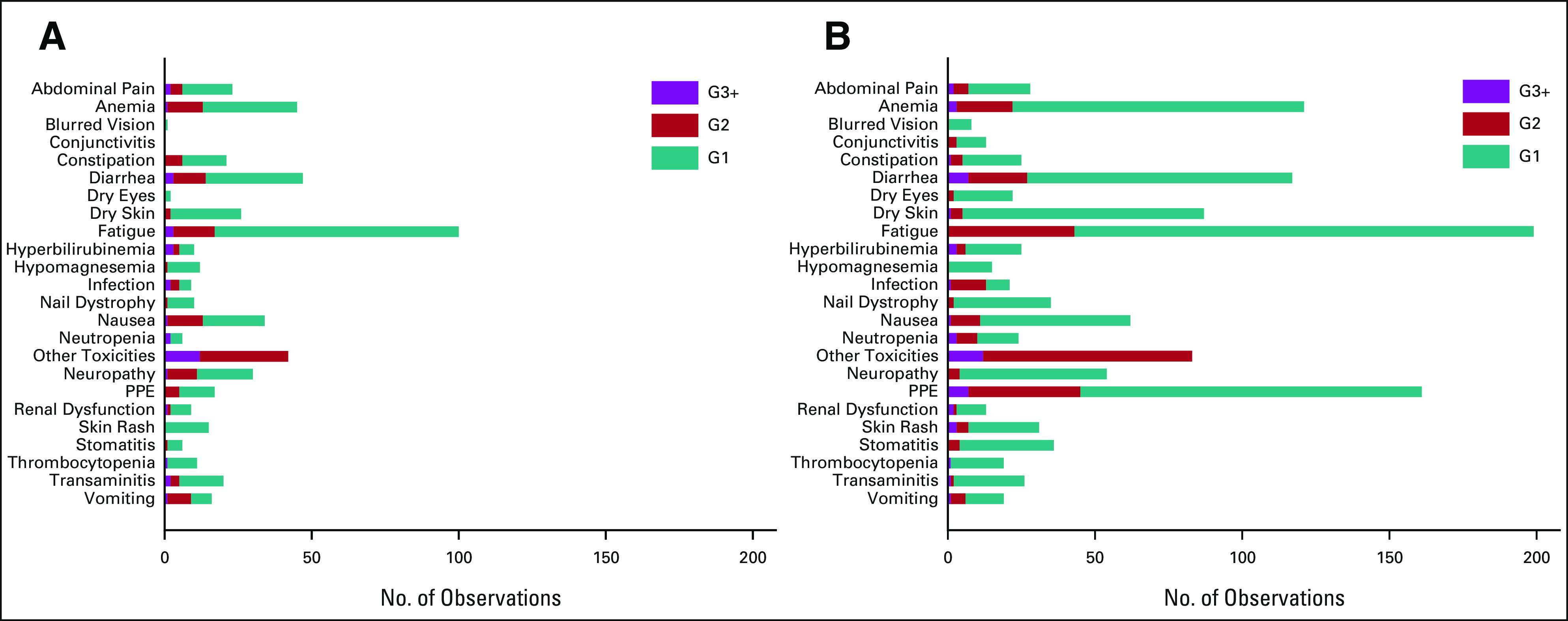
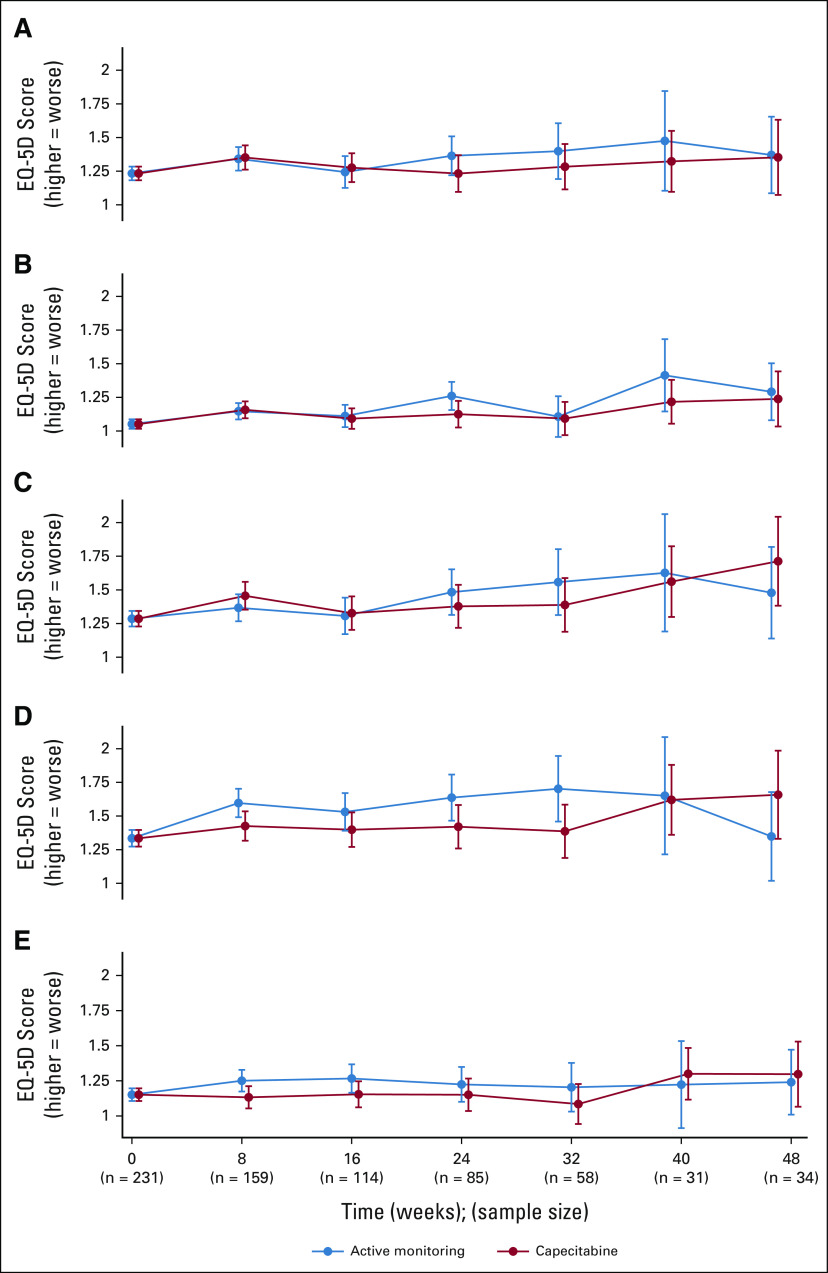
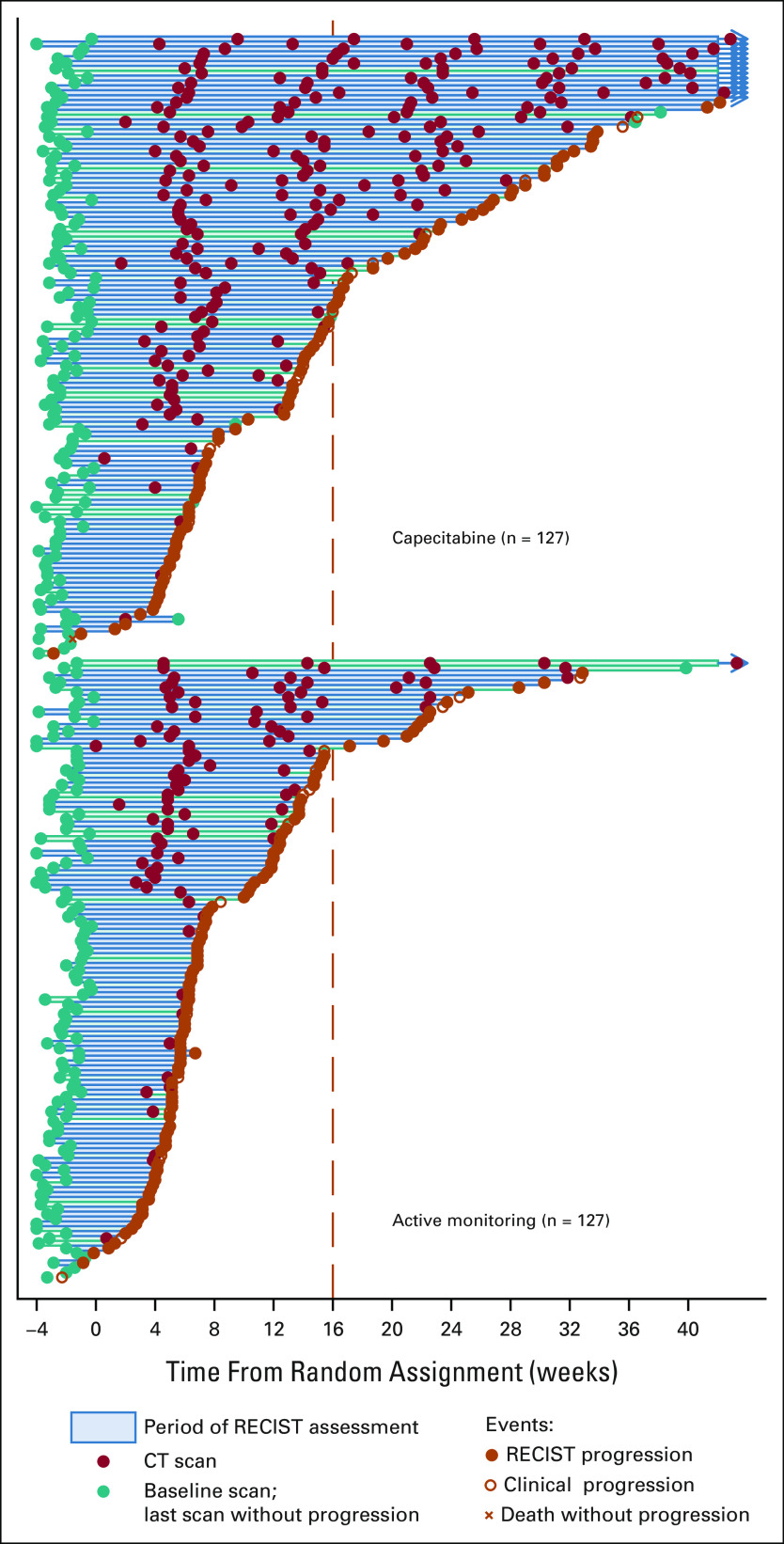
Results: Between March 2014 and March 2020, 254 patients were randomly assigned (127 to capecitabine and 127 to AM) across 88 UK sites. Baseline characteristics were balanced. There was strong evidence of efficacy for PFS (hazard ratio = 0.40; 95% CI, 0.21 to 0.75; P < .0001), but no significant improvement in OS (hazard ratio, 0.93; 95% CI, 0.69 to 1.27; P = .66) was observed. Compliance with treatment was good, and toxicity from capecitabine versus AM was as expected with grade ≥ 2 fatigue (25% v 12%), diarrhea (23% v 13%), and hand-foot syndrome (26% v 3%). Quality of life showed little difference between the groups.
Conclusion: Despite strong evidence of disease control with maintenance therapy, OS remains unaffected and FOCUS4-N provides additional evidence to support the use of treatment breaks as safe management alternatives for patients who are stable or responding to first-line treatment for mCRC. Capecitabine without bevacizumab may be used to extend PFS in the interval after 16 weeks of first-line therapy.
Conflict of interest statement
Figures
Comment in
-
Treatment Holidays for Patients With Metastatic Colorectal Cancer.J Clin Oncol. 2021 Nov 20;39(33):3656-3659. doi: 10.1200/JCO.21.01999. Epub 2021 Sep 13. J Clin Oncol. 2021. PMID: 34516761 No abstract available.
-
Reply to A. Kurreck et al and M.S. Copur et al.J Clin Oncol. 2022 Apr 10;40(11):1263-1264. doi: 10.1200/JCO.21.02806. Epub 2022 Feb 22. J Clin Oncol. 2022. PMID: 35192371 No abstract available.
-
Efficacy, Molecular Biology, Quality of Life, or Economic Aspects: What Do We Really FOCUS oN?J Clin Oncol. 2022 Apr 10;40(11):1260-1262. doi: 10.1200/JCO.21.02310. Epub 2022 Feb 22. J Clin Oncol. 2022. PMID: 35192389 No abstract available.
-
Treatment Break Versus Maintenance in Metastatic Colorectal Cancer.J Clin Oncol. 2022 Apr 10;40(11):1262-1263. doi: 10.1200/JCO.21.02420. Epub 2022 Feb 22. J Clin Oncol. 2022. PMID: 35192401 No abstract available.
References
-
- NCCN . NCCN Guidelines for Patients: Colon Cancer. https://www2.tri-kobe.org/nccn/guideline/colorectal/english/colon.pdf
-
- Van Cutsem E, Cervantes A, Adam R, et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol. 2016;27:1386–1422. - PubMed
-
- Simkens LH, van Tinteren H, May A, et al. Maintenance treatment with capecitabine and bevacizumab in metastatic colorectal cancer (CAIRO3): A phase 3 randomised controlled trial of the Dutch Colorectal Cancer Group. Lancet. 2015;385:1843–1852. - PubMed
-
- Hegewisch-Becker S, Graeven U, Lerchenmuller CA, et al. Maintenance strategies after first-line oxaliplatin plus fluoropyrimidine plus bevacizumab for patients with metastatic colorectal cancer (AIO 0207): A randomised, non-inferiority, open-label, phase 3 trial. Lancet Oncol. 2015;16:1355–1369. - PubMed
