

Myocardial extracellular volume by T1 mapping: a new marker of arrhythmia in mitral valve prolapse
- PMID: 34517908
- PMCID: PMC8438990
- DOI: 10.1186/s12968-021-00797-2
Myocardial extracellular volume by T1 mapping: a new marker of arrhythmia in mitral valve prolapse
Abstract
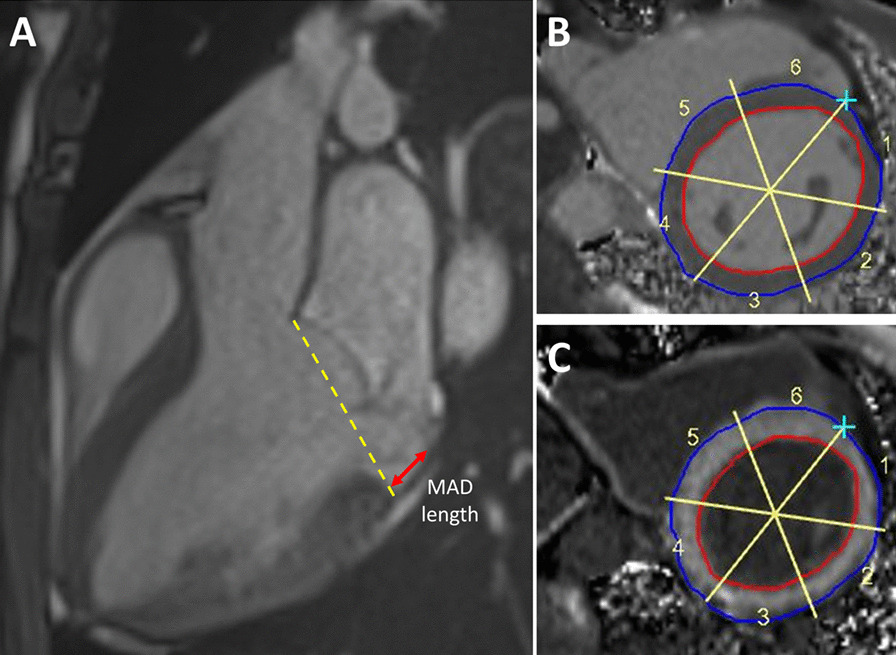
Objectives: We aimed to evaluate the relationship between mitral annular disjunction (MAD) severity and myocardial interstitial fibrosis at the left ventricular (LV) base in patients with mitral valve prolapse (MVP), and to assess the association between severity of interstitial fibrosis and the occurrence of ventricular arrhythmic events.
Background: In MVP, MAD has been associated with myocardial replacement fibrosis and arrhythmia, but the importance of interstitial fibrosis remains unknown.
Methods: In this retrospective study, 30 patients with MVP and MAD (MVP-MAD) underwent cardiovascular magnetic resonance (CMR) with assessment of MAD length, late gadolinium enhancement (LGE), and basal segments myocardial extracellular volume (ECVsyn). The control group included 14 patients with mitral regurgitation (MR) but no MAD (MR-NoMAD) and 10 patients with normal CMR (NoMR-NoMAD). Fifteen MVP-MAD patients underwent 24 h-Holter monitoring.
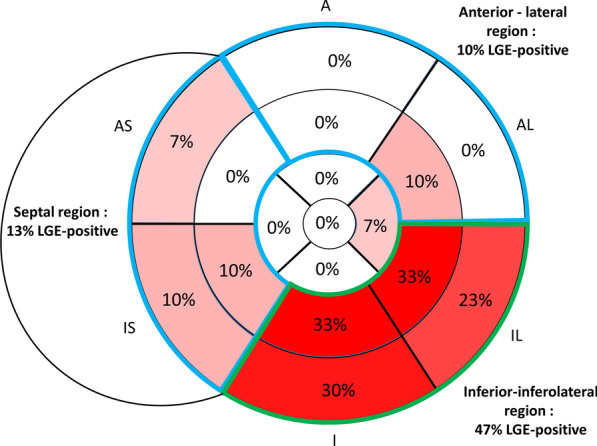
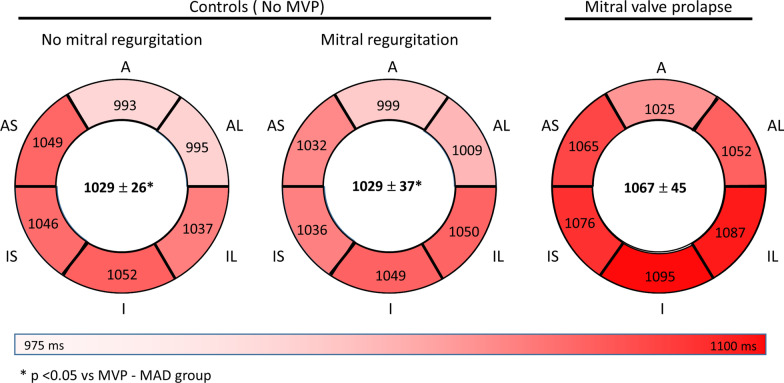
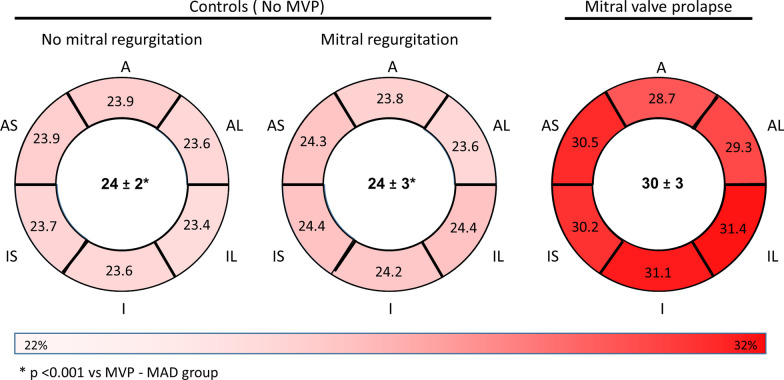
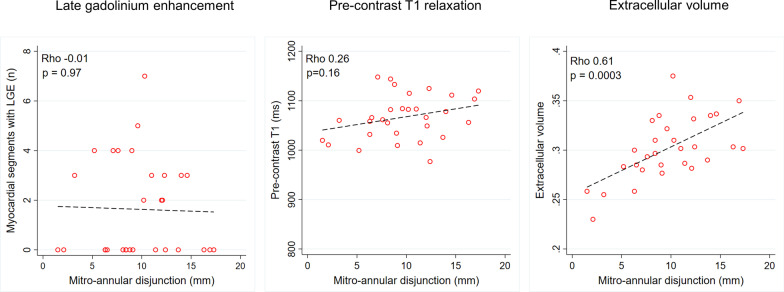
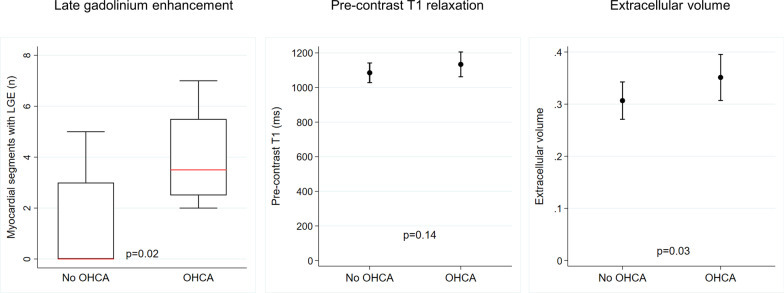
Results: LGE was observed in 47% of MVP-MAD patients and was absent in all controls. ECVsyn was higher in MVP-MAD (30 ± 3% vs 24 ± 3% MR-NoMAD, p < 0.001 and vs 24 ± 2% NoMR-NoMAD, p < 0.001), even in MVP-MAD patients without LGE (29 ± 3% vs 24 ± 3%, p < 0.001 and vs 24 ± 2%, p < 0.001, respectively). MAD length correlated with ECVsyn (rho = 0.61, p < 0.001), but not with LGE extent. Four patients had history of out-of-hospital cardiac arrest; LGE and ECVsyn were equally performant to identify those high-risk patients, area under the receiver operating characteristic (ROC) curve 0.81 vs 0.83, p = 0.84). Among patients with Holter, 87% had complex ventricular arrhythmia. ECVsyn was above the cut-off value in all while only 53% had LGE.
Conclusion: Increase in ECVsyn, a marker of interstitial fibrosis, occurs in MVP-MAD even in the absence of LGE, and was correlated with MAD length and increased risk of out-of-hospital cardiac arrest. ECV should be includedin the CMR examination of MVP patients in an effort to better assess fibrous remodelling as it may provide additional value beyond the assessment of LGE in the arrhythmic risk stratification.
Keywords: Cardiovascular magnetic resonance; Interstitial fibrosis; Mitral annular disjunction; Mitral valve prolapse.
© 2021. The Author(s).
Conflict of interest statement
Beyond the study’s interests, Dr. Le Bloa received a training scholarship from the SIPCA Foundation, Prilly, Switzerland. Prof Schwitter received research grants from Bayer Healthcare, Switzerland. Other authors have nothing to disclose.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
