

Pelvic exenteration for recurrent or persistent gynecologic malignancies: Clinical and histopathologic factors predicting recurrence and survival in a modern cohort
- PMID: 34518053
- PMCID: PMC8585715
- DOI: 10.1016/j.ygyno.2021.08.033
Pelvic exenteration for recurrent or persistent gynecologic malignancies: Clinical and histopathologic factors predicting recurrence and survival in a modern cohort
Abstract
Objectives: To explore pre-operative factors and their impact on overall survival (OS) in a modern cohort of patients who underwent pelvic exenteration (PE) for gynecologic malignancies.
Methods: A retrospective review was performed for all patients who underwent a PE from 1/1/2010 through 12/31/2018 at our institution. Inclusion criteria were exenteration due to recurrent or progressive carcinoma of the uterus, cervix, vagina or vulva, with histologically confirmed complete surgical resection of the malignancy. Exclusion criteria included PE for palliation of symptoms without recurrence, and for ovarian or rare histologic malignancies. Univariable and multivariable analysis were performed to identify factors predicting prolonged survival.
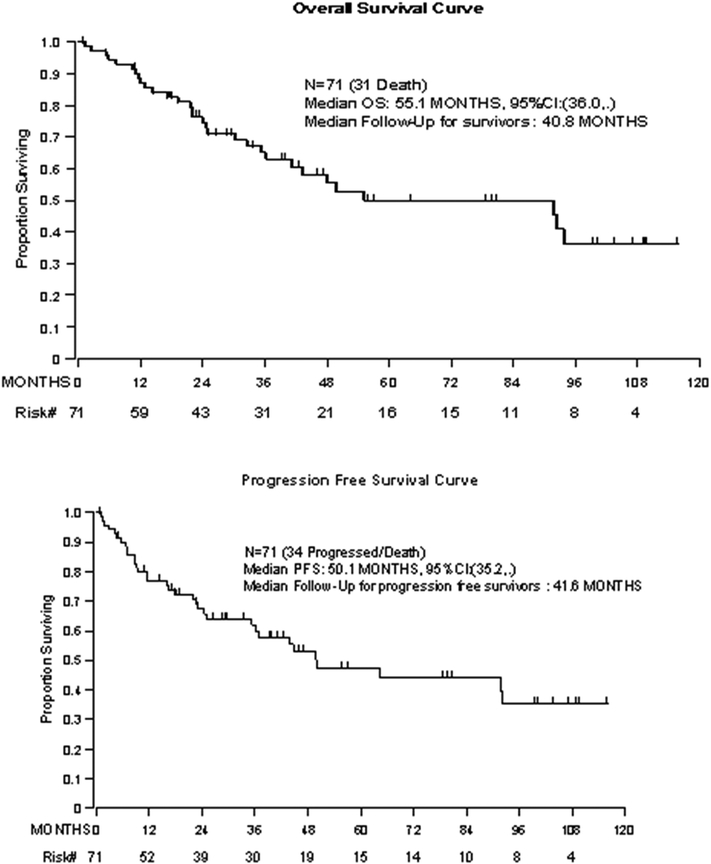
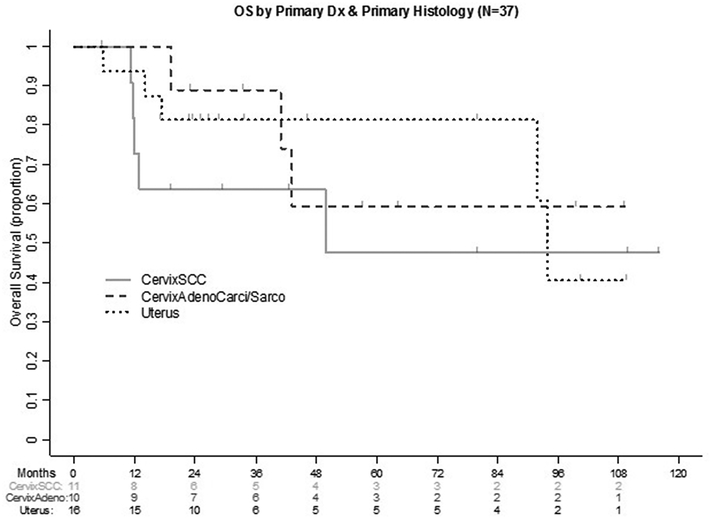
Results: Overall, 71 patients met the inclusion criteria. Median age at time of exenteration was 62 years (range, 28-86 years). Vulvar cancer was the most common primary diagnosis (32%); 30% had cervical cancer; 23%, uterine cancer; 15%, vaginal cancer. Median OS was 55.1 months (95% confidence interval (CI): 36-not estimable) with a median follow-up time of 40.8 months (95% CI: 1-116.1). On univariable analysis, age > 62 years (hazard ratio (HR) 2.71, 95% CI 1.27-5.79), American Society of Anesthesia (ASA) 3-4 (HR: 3.41 (95% CI 1.03-11.29), and vulvar cancer (HR 4.19 (95% CI 1.17-14.96) predicted worse OS. Tumor size and prior progression-free interval (PFI) did not meet statistical significance in OS analyses. On multivariable analysis, there were no significant factors associated with worse OS.
Conclusions: PE performed with curative intent may be considered a treatment option in well-counseled, carefully selected patients, irrespective of tumor size and PFI before exenteration.
Keywords: Gynecologic malignancy; Pelvic exenteration; Recurrent disease.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Brunschwig A. Complete excision of pelvic viscera for advanced carcinoma. A one-stage abdominoperineal operation with end colostomy and bilateral ureteral implantation into the colon above the colostomy. Cancer 1948;1(2):177–183. DOI: 10.1002/1097-0142(194807)1:2<177::AID-CNCR2820010203>3.0.CO;2-A. - DOI - PubMed
-
- Lakhman Y, Nougaret S, Miccò M, et al. Role of MR Imaging and FDG PET/CT in Selection and Follow-up of Patients Treated with Pelvic Exenteration for Gynecologic Malignancies. Radiographics : a review publication of the Radiological Society of North America, Inc 2015;35(4):1295–1313. (In eng). DOI: 10.1148/rg.2015140313. - DOI - PMC - PubMed
-
- Shingleton HM, Soong S-J, Gelder MS, Hatch KD, Baker VV, Austin MJ. Clinical and Histopathologic Factors Predicting Recurrence and Survival After Pelvic Exenteration for Cancer of the Cervix. Obstetrics & Gynecology 1989;73(6). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
