

Characterization of KRAS Mutation Subtypes in Non-small Cell Lung Cancer
- PMID: 34518295
- PMCID: PMC9662933
- DOI: 10.1158/1535-7163.MCT-21-0201
Characterization of KRAS Mutation Subtypes in Non-small Cell Lung Cancer
Abstract
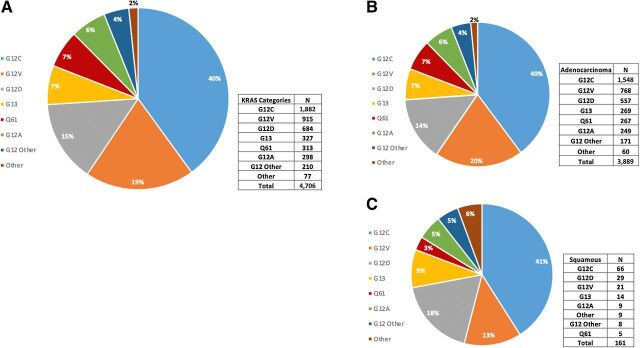
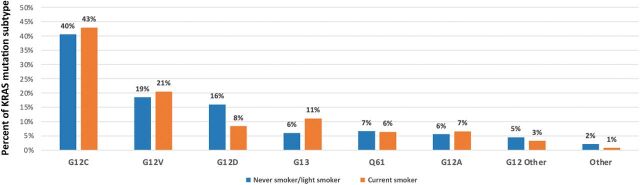
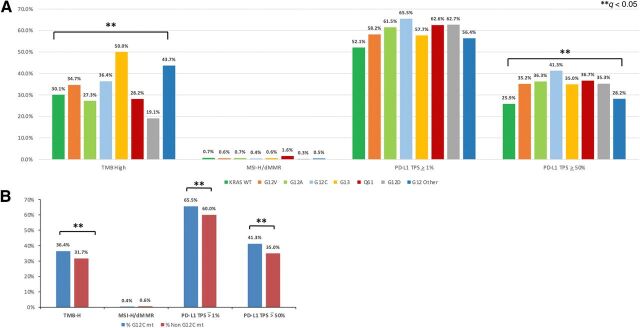
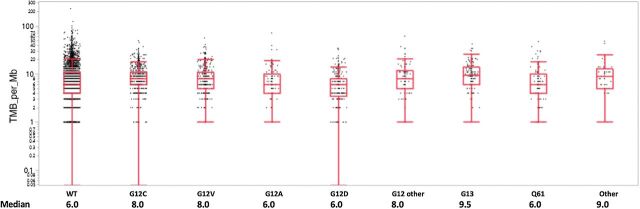
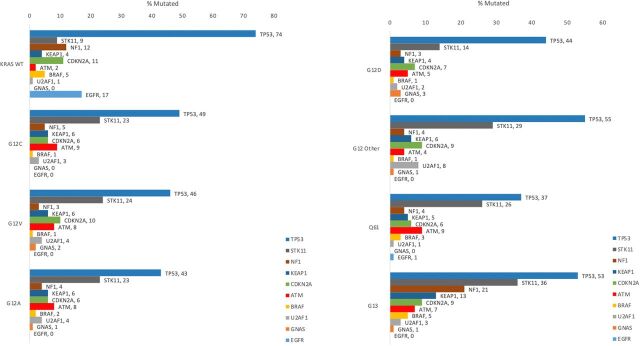
KRAS is the most commonly mutated oncogene in NSCLC and development of direct KRAS inhibitors has renewed interest in this molecular variant. Different KRAS mutations may represent a unique biologic context with different prognostic and therapeutic impact. We sought to characterize genomic landscapes of advanced, KRAS-mutated non-small cell lung cancer (NSCLC) in a large national cohort to help guide future therapeutic development.Molecular profiles of 17,095 NSCLC specimens were obtained using DNA next-generation sequencing of 592 genes (Caris Life Sciences) and classified on the basis of presence and subtype of KRAS mutations. Co-occurring genomic alterations, tumor mutational burden (TMB), and PD-L1 expression [22C3, tumor proportion score (TPS) score] were analyzed by KRAS mutation type.Across the cohort, 4,706 (27.5%) samples harbored a KRAS mutation. The most common subtype was G12C (40%), followed by G12V (19%) and G12D (15%). The prevalence of KRAS mutations was 37.2% among adenocarcinomas and 4.4% in squamous cell carcinomas. Rates of high TMB (≥10 mutations/Mb) and PD-L1 expression varied across KRAS mutation subtypes. KRAS G12C was the most likely to be PD-L1 positive (65.5% TPS ≥ 1%) and PD-L1 high (41.3% TPS ≥ 50%). STK11 was mutated in 8.6% of KRAS wild-type NSCLC but more frequent in KRAS-mutant NSCLC, with the highest rate in G13 (36.2%). TP53 mutations were more frequent in KRAS wild-type NSCLC (73.6%).KRAS mutation subtypes have different co-occurring mutations and a distinct genomic landscape. The clinical relevance of these differences in the context of specific therapeutic interventions warrants investigation.
©2021 The Authors; Published by the American Association for Cancer Research.
Figures
Comment in
- Mol Cancer Ther. 20:2315.
- Mol Cancer Ther. 20:2315.
References
-
- Kris MG, Johnson BE, Kwiatkowski DJ, Iafrate AJ, Wistuba II, Aronson SL, et al. Identification of driver mutations in tumor specimens from 1,000 patients with lung adenocarcinoma: The NCI's Lung Cancer Mutation Consortium (LCMC). J Clin Oncol 2011;29:CRA7506.
-
- Shepherd FA, Domerg C, Hainaut P, Janne PA, Pignon JP, Graziano S, et al. Pooled analysis of the prognostic and predictive effects of KRAS mutation status and KRAS mutation subtype in early-stage resected non-small-cell lung cancer in four trials of adjuvant chemotherapy. J Clin Oncol 2013;31:2173–81. - PMC - PubMed
-
- Rodenhuis S, Boerrigter L, Top B, Slebos RJ, Mooi WJ, van't Veer L, et al. Mutational activation of the K-ras oncogene and the effect of chemotherapy in advanced adenocarcinoma of the lung: a prospective study. J Clin Oncol 1997;15:285–91. - PubMed
-
- Kalikaki A, Koutsopoulos A, Hatzidaki D, Trypaki M, Kontopodis E, Stathopoulos E, et al. Clinical outcome of patients with non-small cell lung cancer receiving front-line chemotherapy according to EGFR and K-RAS mutation status. Lung Cancer 2010;69:110–5. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
