

Minimum Threshold of Bariatric Surgical Weight Loss for Initial Diabetes Remission
- PMID: 34518376
- PMCID: PMC8753771
- DOI: 10.2337/dc21-0714
Minimum Threshold of Bariatric Surgical Weight Loss for Initial Diabetes Remission
Abstract
Objective: There are few studies testing the amount of weight loss necessary to achieve initial remission of type 2 diabetes mellitus (T2DM) following bariatric surgery and no published studies with use of weight loss to predict initial T2DM remission in sleeve gastrectomy (SG) patients.
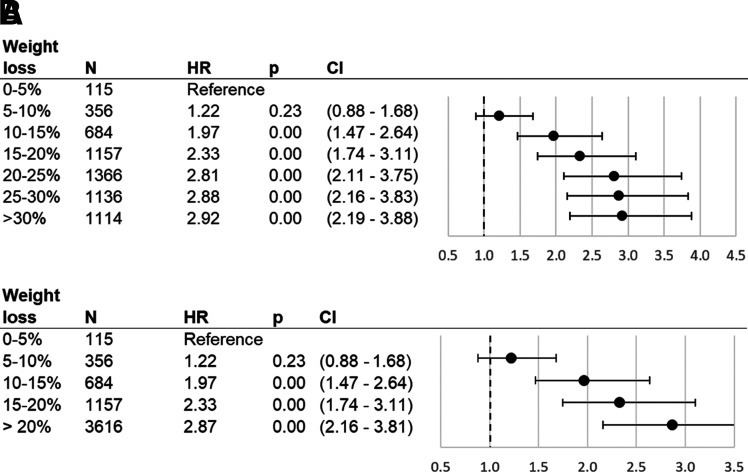
Research design and methods: With Cox proportional hazards models we examined the relationship between initial T2DM remission and percent total weight loss (%TWL) after bariatric surgery. Categories of %TWL were included in the model as time-varying covariates.
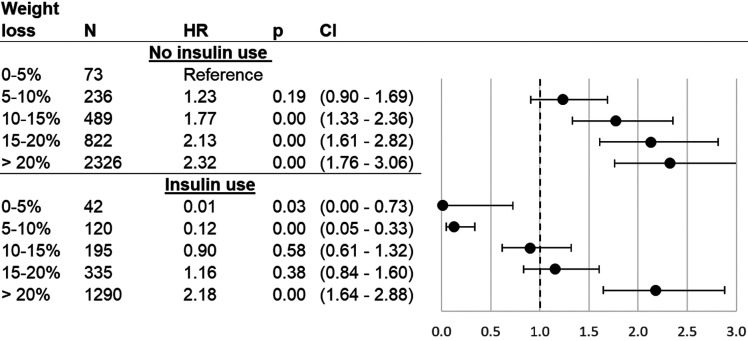
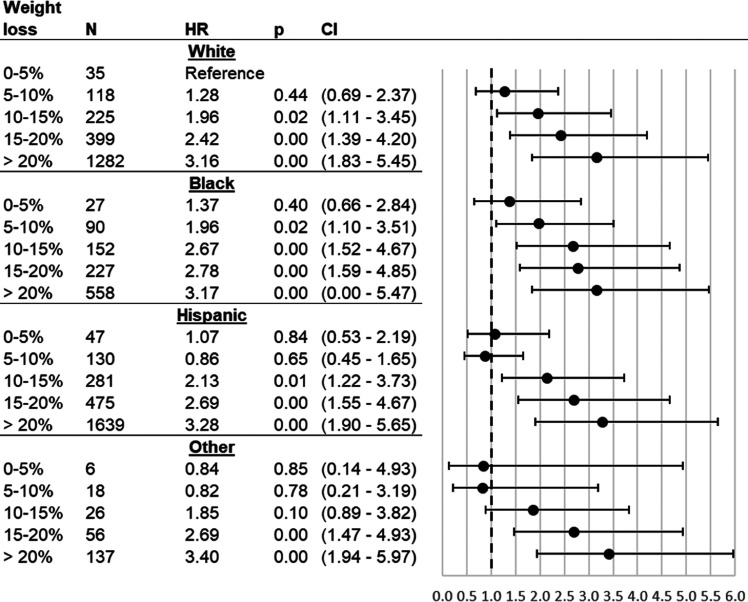
Results: Of patients (N = 5,928), 73% were female; mean age was 49.8 ± 10.3 years and BMI 43.8 ± 6.92 kg/m2, and 57% had Roux-en-Y gastric bypass (RYGB). Over an average follow-up of 5.9 years, 71% of patients experienced initial remission of T2DM (mean time to remission 1.0 year). With 0-5% TWL used as the reference group in Cox proportional hazards models, patients were more likely to remit with each 5% increase in TWL until 20% TWL (hazard ratio range 1.97-2.92). When categories >25% TWL were examined, all patients had a likelihood of initial remission similar to that of 20-25% TWL. Patients who achieved >20% TWL were more likely to achieve initial T2DM remission than patients with 0-5% TWL, even if they were using insulin at the time of surgery.
Conclusions: Weight loss after bariatric surgery is strongly associated with initial T2DM remission; however, above a threshold of 20% TWL, rates of initial T2DM remission did not increase substantially. Achieving this threshold is also associated with initial remission even in patients who traditionally experience lower rates of remission, such as patients taking insulin.
© 2021 by the American Diabetes Association.
Figures
Comment in
-
Weighing in on Type 2 Diabetes Remission.Diabetes Care. 2022 Jan 1;45(1):28-30. doi: 10.2337/dci21-0041. Diabetes Care. 2022. PMID: 34986262 No abstract available.
References
-
- Arterburn DE, Telem DA, Kushner RF, Courcoulas AP. Benefits and risks of bariatric surgery in adults: a review. JAMA 2020;324:879–887 - PubMed
-
- van de Laar AWJM, Acherman YIZ. Weight loss percentile charts of large representative series: a benchmark defining sufficient weight loss challenging current criteria for success of bariatric surgery. Obes Surg 2014;24:727–734 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
