

Impact of enzalutamide on patient-reported fatigue in patients with prostate cancer: data from the pivotal clinical trials
- PMID: 34518652
- PMCID: PMC9184276
- DOI: 10.1038/s41391-021-00447-9
Impact of enzalutamide on patient-reported fatigue in patients with prostate cancer: data from the pivotal clinical trials
Abstract
Background: Fatigue is a multifactorial symptom commonly reported by patients with prostate cancer as a result of disease and treatment. This study assesses the impact enzalutamide has on patient-reported fatigue ("fatigue") by using patient-reported outcomes from four pivotal, placebo-controlled trials of enzalutamide (ARCHES (NCT02677896), PROSPER (NCT02003924), PREVAIL (NCT01212991), and AFFIRM (NCT00974311)).
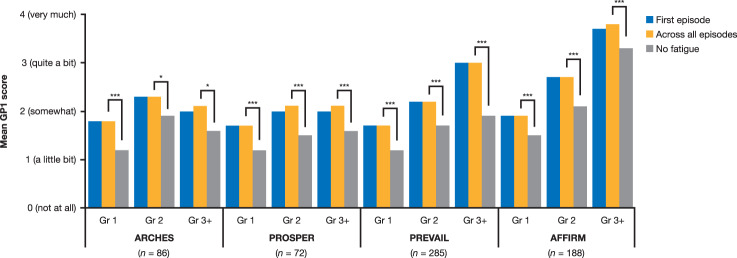
Methods: Fatigue was assessed in the individual studies using the Functional Assessment of Cancer Therapy-Prostate item GP1 at baseline, weeks 13 or 17, and every 12 weeks until disease progression. Longitudinal changes were assessed using mean scores and mixed-model repeated measures.
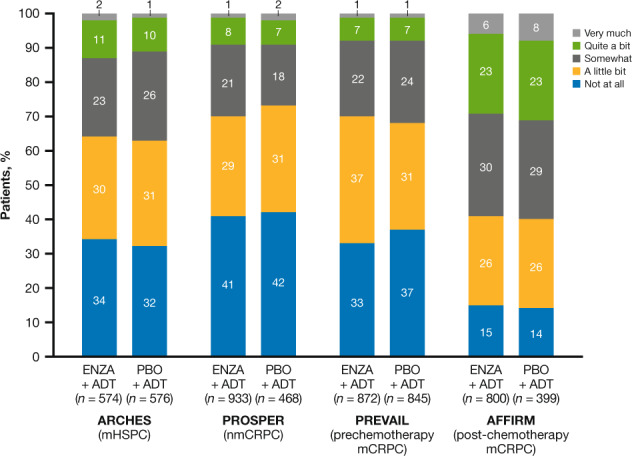
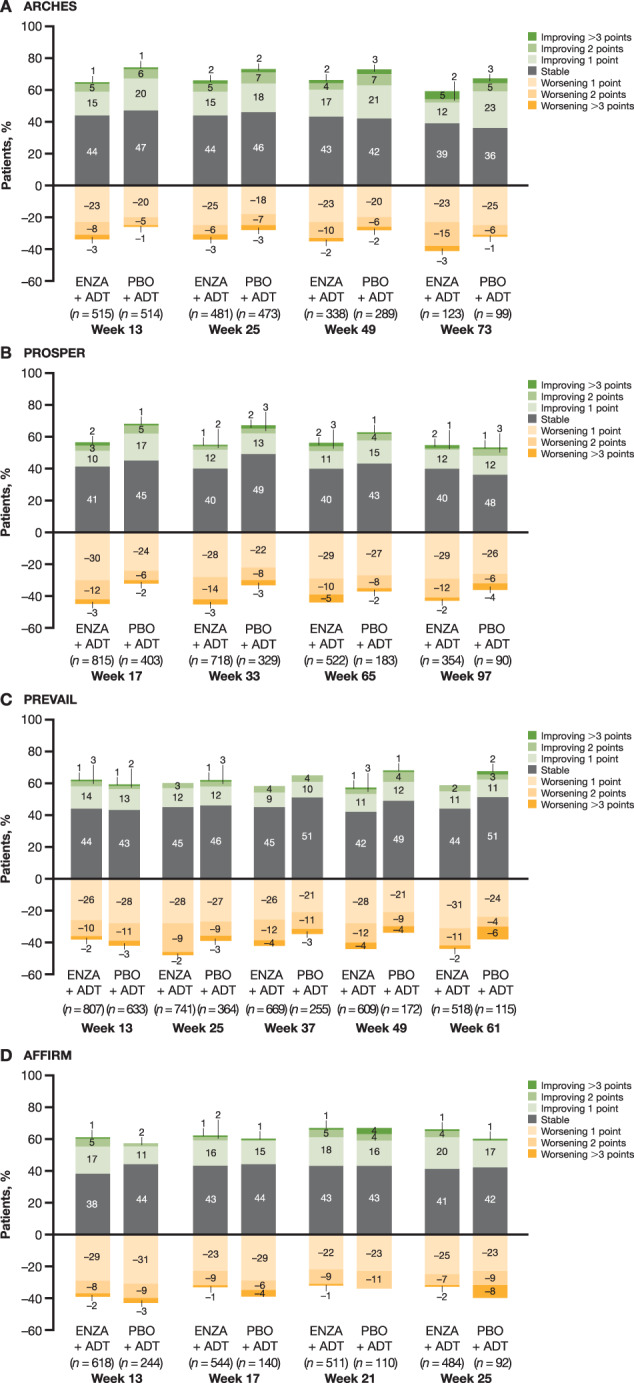
Results: The fatigue rates at baseline were higher in patients with later-stage disease (metastatic and/or castration-resistant prostate cancer (CRPC)) and among patients who had already received prior treatment lines; rates ranged between 58% in PROSPER (nonmetastatic CRPC) and 86% in AFFIRM (post-docetaxel metastatic CRPC). Irrespective of disease state, initiation of enzalutamide or placebo resulted in an early increase of fatigue (by weeks 13 or 17), with fatigue levels stabilizing thereafter. At last assessment, ≥55% of patients reported fatigue improvement or stabilization in all trials compared to baseline. More patients reported fatigue worsening by ≥1 or ≥2 units with enzalutamide plus androgen deprivation therapy (ADT) than with placebo plus ADT in ARCHES, PROSPER, and PREVAIL, but the between-group difference was <10% in all trials.
Conclusions: The levels of fatigue were greater in mCRPC and lower in earlier states of disease. In all trials, patients reported a small increase in fatigue for the first 13-17 weeks after starting enzalutamide or placebo, with slightly greater fatigue with enzalutamide in all studies except AFFIRM, but fatigue stabilized or improved thereafter. This suggests a role for clinical management of fatigue to help patients cope early in treatment.
© 2021. The Author(s).
Conflict of interest statement
BFT has received grants or contracts, consulting fees, and payment or honoraria for lectures, presentations, speaker bureaus, publication writing, or educational events from Amgen, Astellas, Bayer, Janssen, Myovant, Novartis (Advanced Accelerator Applications), and Sanofi and payment for expert testimony from Tookad. SJF has received consulting fees from Astellas, AstraZeneca, Bayer, Clovis, Janssen, Merck, Myovant, Pfizer, and Sanofi and payment for lectures, presentations, speaker bureaus, publication writing, or education events from AstraZeneca and Sanofi. AJA has received research funding from AstraZeneca, Bayer, Bristol Myers Squibb, Clovis, Constellation, Dendreon, Janssen, Medivation, Merck, Novartis, Pfizer, Roche/Genentech, and Sanofi, consulting fees from Astellas, AstraZeneca, Bayer, Dendreon, Janssen, Medivation, Merck, Novartis, Pfizer, and Sanofi, payment or honoraria for lectures, presentations, speaker bureaus, publication writing, or educational events from Bayer and Dendreon, and support for attending meetings and/or travel from Bayer, Dendreon, and Janssen. TMB has received consulting fees from Arvinas, Astellas, AstraZeneca, Bayer, Bristol Myers Squibb, Clovis, Constellation, GlaxoSmithKline, Grail, Janssen, Merck, Myovant, Novartis, Pfizer, Sanofi, and Tolero and owns stock or stock options in Arvinas and Salarius; his institution has received grants or contracts from Alliance Foundation Trials, Bayer, Boehringer Ingelheim, Corcept, Endocyte/Advanced Accelerator Applications, Freenome, Grail, Harpoon, Janssen, Medivation, Sotio, Theraclone Sciences/OncoResponse, and Zenith Epigenetics. AS has received research grants from Amgen, Immatics Biotechnologies GmbH, Karl Storz AG, and Novartis AG, consulting fees from Alere, Ipsen, Janssen, and Roche, payment or honoraria as a speaker from Amgen, Astellas, AstraZeneca, CureVac, Ipsen, Janssen, and Sanofi Aventis and for participating in advisory board meetings from Alere, Bristol Myers Squibb, Ferring, Ipsen, Janssen, Roche, Stebabiotech, and Synergo, and served as an investigator in clinical trials sponsored by Bayer AG, Cepheid, CureVac, GenomeDx Biosciences, Immatics Biotechnologies GmbH, Johnson & Johnson, and Roche. CNS has received honoraria for lectures, presentations, speaker bureaus, publication writing, or educational events from Astellas, AstraZeneca, Bristol Myers Squibb, CCO Clinical, Foundation Medicine, Immunomedics (now Gilead), Incyte, Janssen, Medscape, Merck, MSD, NCI, Pfizer, Roche-Genentech, Sanofi-Genzyme, and UroToday and payment or honoraria for participating in advisory board meetings from Impact, NCI, and NeoTx. MH has received contracts for clinical trials from Arvinas, AstraZeneca, Bayer, Genentech, and Pfizer and honoraria for lectures at symposiums from Astellas, AstraZeneca, Merck, and Sanofi/Genzyme and for participating in advisory board meetings from Bayer, Bristol Myers Squibb, Daiichi Sankyo, Genentech, and Janssen. AG, HB, and SH are employees of Astellas. KR is an employee of Pfizer. CI and JT are employees of IQVIA, which received professional service fees from Astellas for conducting the analyses presented here. FS has received consulting fees and payments or honoraria for lectures, presentations, speaker bureaus, publication writing, or educational events from Amgen, Astellas, AstraZeneca, Bayer, Bristol Myers Squibb, Janssen, Merck, Myovant, Pfizer, and Sanofi; his institution has received grants or contracts from Astellas, AstraZeneca, Bayer, Bristol Myers Squibb, Janssen, Merck, Myovant, Pfizer, and Sanofi. In addition, all authors received support from Astellas, in the form of study funding, IQVIA, in the form of study analysis and medical writing, and Complete HealthVizion, in the form of editing of the manuscript.
Figures

References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
