

Short-term outcomes of open surgical abdominal aortic aneurysm repair from the Dutch Surgical Aneurysm Audit
- PMID: 34518868
- PMCID: PMC8438252
- DOI: 10.1093/bjsopen/zrab086
Short-term outcomes of open surgical abdominal aortic aneurysm repair from the Dutch Surgical Aneurysm Audit
Abstract
Background: The sharp decrease in open surgical repair (OSR) for abdominal aortic aneurysm (AAA) has raised concerns about contemporary postoperative outcomes. The study was designed to analyse the impact of complications on clinical outcomes within 30 days following OSR.
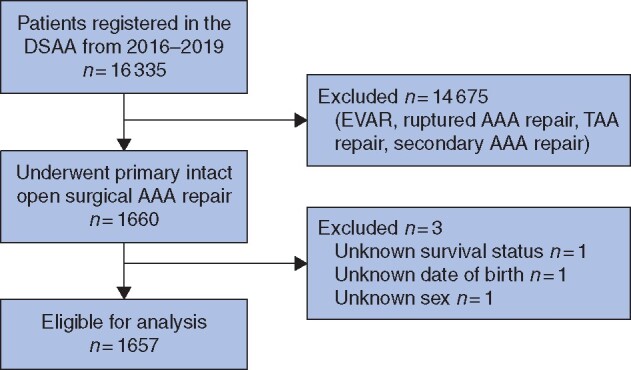
Methods: Patients who underwent OSR for intact AAA registered prospectively between 2016 and 2019 in the Dutch Surgical Aneurysm Audit were included. Complications and outcomes (death, secondary interventions, prolonged hospitalization) were evaluated. The adjusted relative risk (aRr) and 95 per cent confidence intervals were computed using Poisson regression. Subsequently, the population-attributable fraction (PAF) was calculated. The PAF reflects the expected percentage reduction of an outcome if a complication were to be completely prevented.
Results: A total of 1657 patients were analysed. Bowel ischaemia and renal complications had the largest impact on death (aRr 12·44 (95 per cent c.i. 7·95 to 19·84) at PAF 20 (95 per cent c.i. 8·4 to 31·5) per cent and aRr 5·07 (95 per cent c.i. 3·18 to 8.07) at PAF 14 (95 per cent c.i. 0·7 to 27·0) per cent, respectively). Arterial occlusion had the greatest impact on secondary interventions (aRr 11·28 (95 per cent c.i. 8·90 to 14·30) at PAF 21 (95 per cent c.i. 14·7 to 28·1) per cent), and pneumonia (aRr 2·52 (95 per cent c.i. 2·04 to 3·10) at PAF 13 (95 per cent c.i. 8·3 to 17·8) per cent) on prolonged hospitalization. Small effects were observed on outcomes for other complications.
Conclusion: The greatest clinical impact following OSR can be made by focusing on measures to reduce the occurrence of bowel ischaemia, arterial occlusion and pneumonia.
© The Author(s) 2021. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures
References
-
- Mani K, Lees T, Beiles B, Jensen LP, Venermo M, Simo G. et al. Treatment of abdominal aortic aneurysm in nine countries 2005–2009: a Vascunet report. Eur J Vasc Endovasc Surg 2011;42:598–607. - PubMed
-
- Dutch Institute for Clinical Auditing. Dutch Surgical Aneurysm Audit. https://dica.nl/dsaa/home (accessed 3 April 2020).
-
- Lijftogt N, Vahl AC, Wilschut ED, Elsman BHP, Amodio S, van Zwet EW. et al. Adjusted hospital outcomes of abdominal aortic aneurysm surgery reported in the Dutch Surgical Aneurysm Audit. Eur J Vasc Endovasc Surg 2017;53:520–532. - PubMed
-
- Dua A, Kuy S, Lee CJ, Upchurch GR Jr, Desai SS.. Epidemiology of aortic aneurysm repair in the United States from 2000 to 2010. J Vasc Surg 2014;59:1512–1517. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
