

The role of endotheliitis in COVID-19: Real-world experience of 11 190 patients and literature review for a pathophysiological map to clinical categorisation
- PMID: 34519155
- PMCID: PMC8646438
- DOI: 10.1111/ijcp.14843
The role of endotheliitis in COVID-19: Real-world experience of 11 190 patients and literature review for a pathophysiological map to clinical categorisation
Abstract
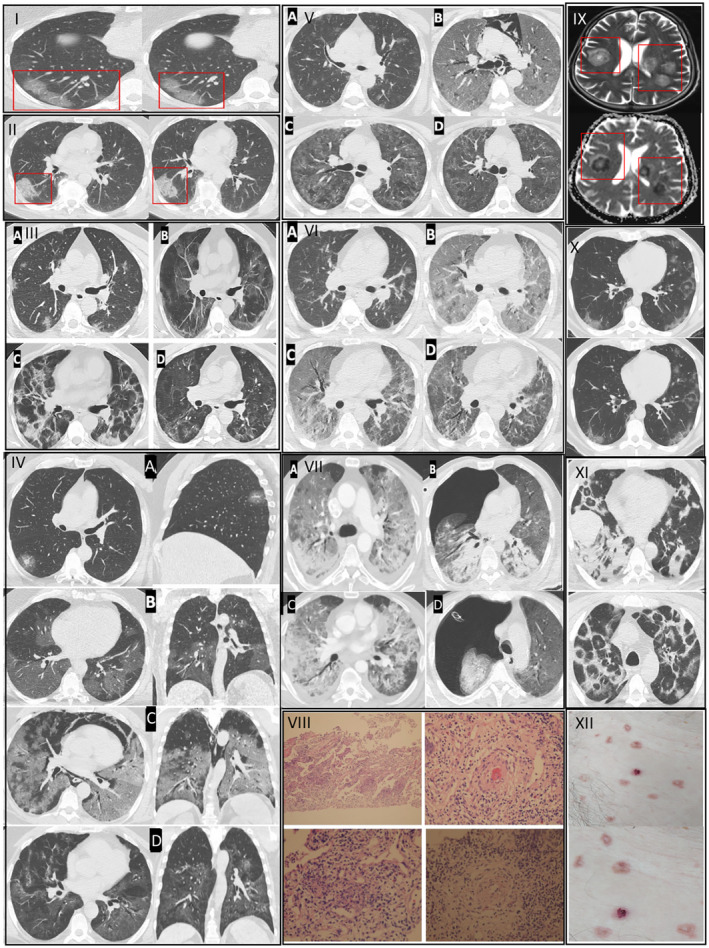
Objective: COVID-19 may yield a variety of clinical pictures, differing from pneumonitis to Acute Respiratory Distress Syndrome along with vascular damage in the lung tissue, named endotheliitis. To date, no specific treatment strategy was approved for the prevention or treatment of COVID-19 in terms of endotheliitis-related comorbidities. Here, we presented our treatment strategies for 11 190 COVID-19 patients depending on categorisation by the severity of both the respiratory and vascular distress and presented the manifestations of endotheliitis in skin, lung and brain tissues according to the different phases of COVID-19.
Methods: After a retrospective examination, patients were divided into three groups according to their repercussions of vascular distress, which were represented by radiological, histopathological and clinical findings. We presented the characteristics and courses of seven representative and complicated cases which demonstrate different phases of the disease and discussed the treatment strategies in each group.
Results: Among 11 190 patients, 9294 patients met the criteria for Group A, and 1376 patients were presented to our clinics with Group B characteristics. Among these patients, 1896 individuals (Group B and Group C) were hospitalised. While 1220 inpatients were hospitalised within the first 10 days after the diagnosis, 676 of them were worsened and hospitalised 10 days after their diagnosis. Among hospitalised patients, 520 of them did not respond to group A and B treatments and developed hypoxemic respiratory failure (Group C) and 146 individuals needed ventilator support and were followed in the intensive care unit, and 43 (2.2%) patients died.
Conclusion: Distinctive manifestations in each COVID-19 patient, including non-respiratory conditions in the acute phase and the emerging risk of long-lasting complications, suggest that COVID-19 has endotheliitis-centred thrombo-inflammatory pathophysiology. Daily evaluation of clinical, laboratory and radiological findings of patients and deciding appropriate pathophysiological treatment would help to reduce the mortality rate of COVID-19.
© 2021 John Wiley & Sons Ltd.
Conflict of interest statement
The authors have declared no disclosures.
Figures
References
-
- Coronavirus update (live)‐worldmeter. www.worldometers.info. Accessed May 11, 2021
-
- Republic of Turkey Ministry of Health . COVID‐19 Interim Guidance (T.C. Sağlık Bakanlığı COVID‐19 (SARS‐CoV‐2 Enfeksiyonu) Rehberi). 2020. https://covid19bilgi.saglik.gov.tr/depo/rehberler/COVID‐19_Rehberi.pdf?t.... Accessed Apr 14, 2020
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous