

Safety and efficacy of different prophylactic anticoagulation dosing regimens in critically and non-critically ill patients with COVID-19: a systematic review and meta-analysis of randomized controlled trials
- PMID: 34519777
- PMCID: PMC8499924
- DOI: 10.1093/ehjcvp/pvab070
Safety and efficacy of different prophylactic anticoagulation dosing regimens in critically and non-critically ill patients with COVID-19: a systematic review and meta-analysis of randomized controlled trials
Abstract
Background: The clinical impact of different prophylactic anticoagulation regimens among hospitalized patients with coronavirus disease 2019 (COVID-19) remains unclear. We pooled evidence from available randomized controlled trials (RCTs) to provide insights on this topic.
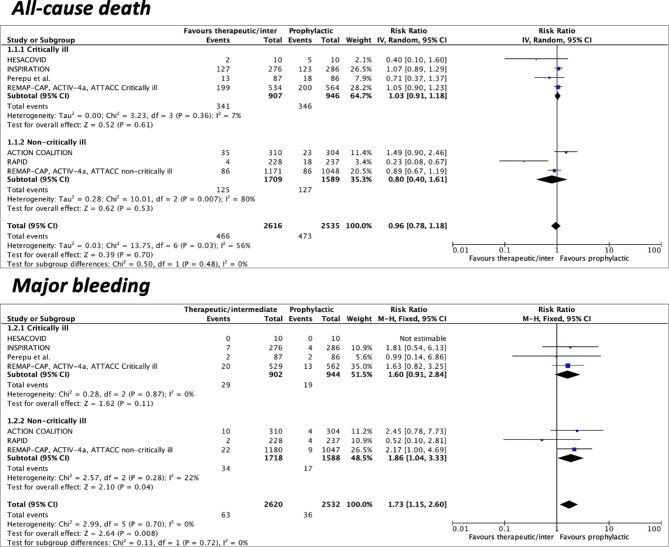
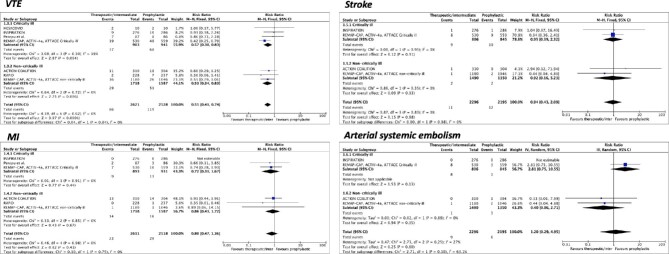
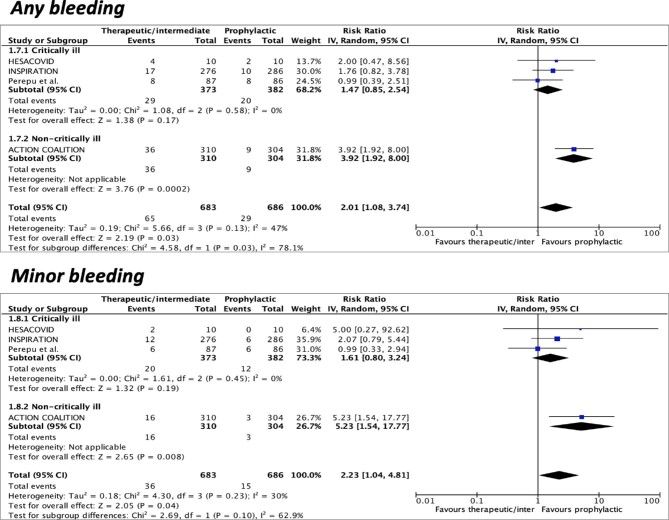
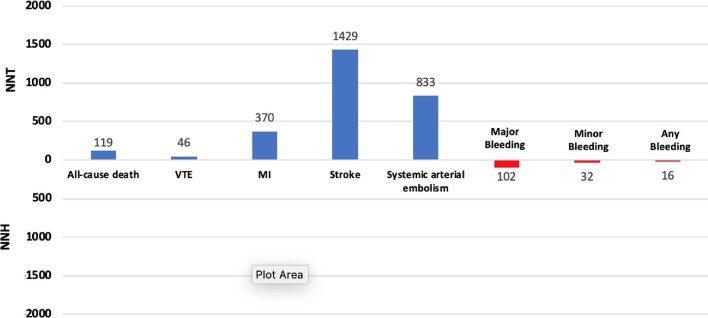
Methods and results: We searched for RCTs comparing treatment with an escalated-dose (intermediate-dose or therapeutic-dose) vs. a standard-dose prophylactic anticoagulation regimen in critically and non-critically ill COVID-19 patients requiring hospitalization and without a formal indication for anticoagulation. The primary efficacy endpoint was all-cause death, and the primary safety endpoint was major bleeding. Seven RCTs were identified, including 5154 patients followed on an average of 33 days. Compared to standard-dose prophylactic anticoagulation, escalated-dose prophylactic anticoagulation was not associated with a reduction of all-cause death [17.8% vs. 18.6%; risk ratio (RR) 0.96, 95% confidence interval (CI) 0.78-1.18] but was associated with an increase in major bleeding (2.4% vs. 1.4%; RR 1.73, 95%CI 1.15-2.60). Compared to prophylactic anticoagulation used at a standard dose, an escalated dose was associated with lower rates of venous thromboembolism (2.5% vs. 4.7%; RR 0.55, 95%CI 0.41-0.74) without a significant effect on myocardial infarction (RR 0.80, 95%CI 0.47-1.36), stroke (RR 0.94, 95%CI 0.43-2.09), or systemic arterial embolism (RR 1.20, 95%CI 0.29-4.95). There were no significant interactions in the subgroup analysis for critically and non-critically ill patients.
Conclusions: Our findings provide comprehensive and high-quality evidence for the use of standard-dose prophylactic anticoagulation over an escalated-dose regimen as routine standard of care for hospitalized patients with COVID-19 who do not have an indication for therapeutic anticoagulation, irrespective of disease severity.
Study registration: This study is registered in PROSPERO (CRD42021257203).
Keywords: Anticoagulant therapy; Bleeding; Coronavirus disease 2019; Death; Thrombosis.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
In COVID-19, escalated- vs. prophylactic-dose anticoagulation does not reduce mortality and increases major bleeding.Ann Intern Med. 2022 Feb;175(2):JC18. doi: 10.7326/J21-0021. Epub 2022 Feb 1. Ann Intern Med. 2022. PMID: 35099996
References
-
- Bikdeli B, Madhavan MV, Jimenez D, Chuich T, Dreyfus I, Driggin E, Nigoghossian C, Ageno W, Madjid M, Guo Y, Tang LV, Hu Y, Giri J, Cushman M, Quere I, Dimakakos EP, Gibson CM, Lippi G, Favaloro EJ, Fareed J, Caprini JA, Tafur AJ, Burton JR, Francese DP, Wang EY, Falanga A, McLintock C, Hunt BJ, Spyropoulos AC, Barnes GD, Eikelboom JW, Weinberg I, Schulman S, Carrier M, Piazza G, Beckman JA, Steg PG, Stone GW, Rosenkranz S, Goldhaber SZ, Parikh SA, Monreal M, Krumholz HM, Konstantinides SV, Weitz JI, Lip GYH, Global Covid-19 Thrombosis Collaborative Group EbtINE, the Iua SbtESCWGoPC, Right Ventricular F . COVID-19 and thrombotic or thromboembolic disease: implications for prevention, antithrombotic therapy, and follow-up: JACC state-of-the-art review. J Am Coll Cardiol 2020;75:2950–2973. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
