

Effect of Urate-Elevating Inosine on Early Parkinson Disease Progression: The SURE-PD3 Randomized Clinical Trial
- PMID: 34519802
- PMCID: PMC8441591
- DOI: 10.1001/jama.2021.10207
Effect of Urate-Elevating Inosine on Early Parkinson Disease Progression: The SURE-PD3 Randomized Clinical Trial
Abstract
Importance: Urate elevation, despite associations with crystallopathic, cardiovascular, and metabolic disorders, has been pursued as a potential disease-modifying strategy for Parkinson disease (PD) based on convergent biological, epidemiological, and clinical data.
Objective: To determine whether sustained urate-elevating treatment with the urate precursor inosine slows early PD progression.
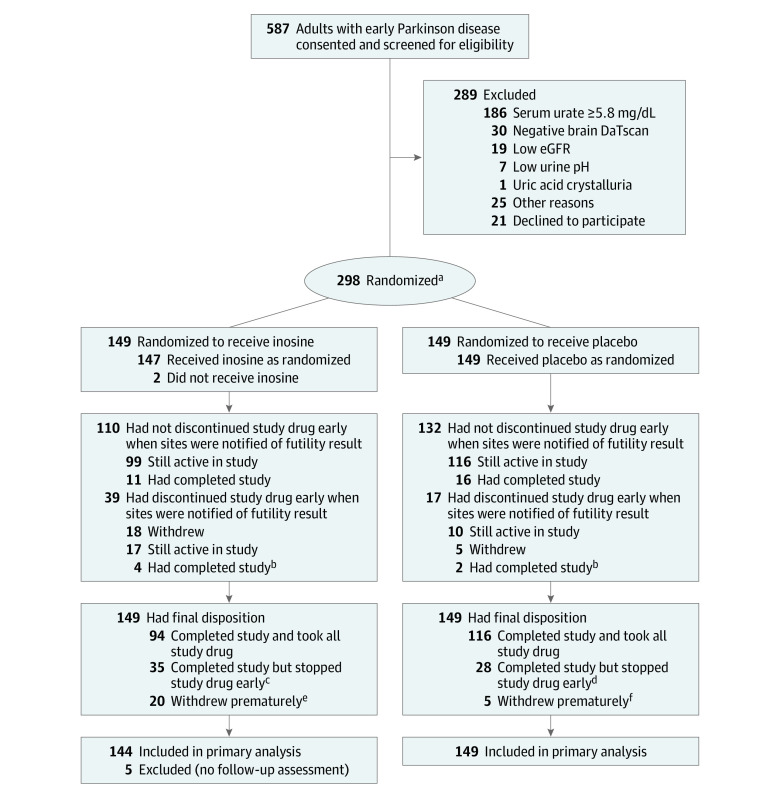
Design, participants, and setting: Randomized, double-blind, placebo-controlled, phase 3 trial of oral inosine treatment in early PD. A total of 587 individuals consented, and 298 with PD not yet requiring dopaminergic medication, striatal dopamine transporter deficiency, and serum urate below the population median concentration (<5.8 mg/dL) were randomized between August 2016 and December 2017 at 58 US sites, and were followed up through June 2019.
Interventions: Inosine, dosed by blinded titration to increase serum urate concentrations to 7.1-8.0 mg/dL (n = 149) or matching placebo (n = 149) for up to 2 years.
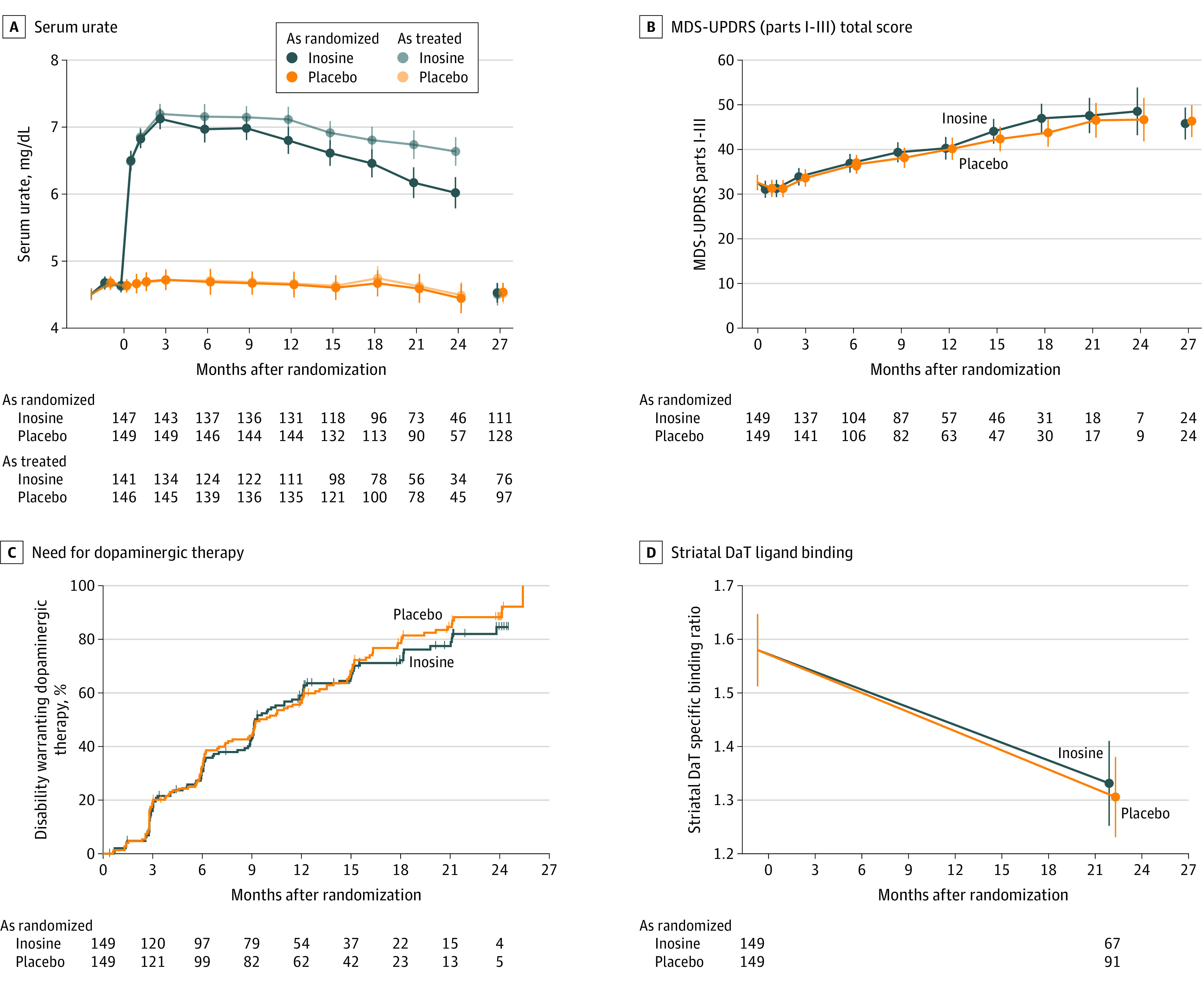
Main outcomes and measures: The primary outcome was rate of change in the Movement Disorder Society Unified Parkinson Disease Rating Scale (MDS-UPDRS; parts I-III) total score (range, 0-236; higher scores indicate greater disability; minimum clinically important difference of 6.3 points) prior to dopaminergic drug therapy initiation. Secondary outcomes included serum urate to measure target engagement, adverse events to measure safety, and 29 efficacy measures of disability, quality of life, cognition, mood, autonomic function, and striatal dopamine transporter binding as a biomarker of neuronal integrity.
Results: Based on a prespecified interim futility analysis, the study closed early, with 273 (92%) of the randomized participants (49% women; mean age, 63 years) completing the study. Clinical progression rates were not significantly different between participants randomized to inosine (MDS-UPDRS score, 11.1 [95% CI, 9.7-12.6] points per year) and placebo (MDS-UPDRS score, 9.9 [95% CI, 8.4-11.3] points per year; difference, 1.26 [95% CI, -0.59 to 3.11] points per year; P = .18). Sustained elevation of serum urate by 2.03 mg/dL (from a baseline level of 4.6 mg/dL; 44% increase) occurred in the inosine group vs a 0.01-mg/dL change in serum urate in the placebo group (difference, 2.02 mg/dL [95% CI, 1.85-2.19 mg/dL]; P<.001). There were no significant differences for secondary efficacy outcomes including dopamine transporter binding loss. Participants randomized to inosine, compared with placebo, experienced fewer serious adverse events (7.4 vs 13.1 per 100 patient-years) but more kidney stones (7.0 vs 1.4 stones per 100 patient-years).
Conclusions and relevance: Among patients recently diagnosed as having PD, treatment with inosine, compared with placebo, did not result in a significant difference in the rate of clinical disease progression. The findings do not support the use of inosine as a treatment for early PD.
Trial registration: ClinicalTrials.gov Identifier: NCT02642393.
Conflict of interest statement
Figures
Comment in
-
Effect of Urate-Elevating Inosine on Progression of Early Parkinson Disease.JAMA. 2022 Jan 4;327(1):85. doi: 10.1001/jama.2021.21008. JAMA. 2022. PMID: 34982123 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
