

Identification of a Rule to Predict Response to Sarilumab in Patients with Rheumatoid Arthritis Using Machine Learning and Clinical Trial Data
- PMID: 34519964
- PMCID: PMC8572308
- DOI: 10.1007/s40744-021-00361-5
Identification of a Rule to Predict Response to Sarilumab in Patients with Rheumatoid Arthritis Using Machine Learning and Clinical Trial Data
Erratum in
-
Correction to: Identification of a Rule to Predict Response to Sarilumab in Patients with Rheumatoid Arthritis Using Machine Learning and Clinical Trial Data.Rheumatol Ther. 2021 Dec;8(4):1921-1922. doi: 10.1007/s40744-021-00389-7. Rheumatol Ther. 2021. PMID: 34714512 Free PMC article. No abstract available.
Abstract
Introduction: In rheumatoid arthritis, time spent using ineffective medications may lead to irreversible disease progression. Despite availability of targeted treatments, only a minority of patients achieve sustained remission, and little evidence exists to direct the choice of biologic disease-modifying antirheumatic drugs in individual patients. Machine learning was used to identify a rule to predict the response to sarilumab and discriminate between responses to sarilumab versus adalimumab, with a focus on clinically feasible blood biomarkers.
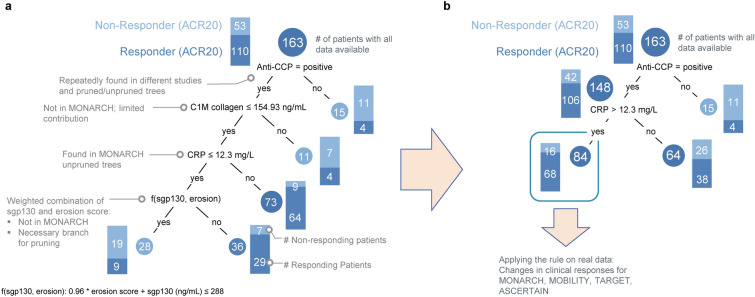
Methods: The decision tree model GUIDE was trained using a data subset from the sarilumab trial with the most biomarker data, MOBILITY, to identify a rule to predict disease activity after sarilumab 200 mg. The training set comprised 18 categorical and 24 continuous baseline variables; some data were omitted from training and used for validation by the algorithm (cross-validation). The rule was tested using full datasets from four trials (MOBILITY, MONARCH, TARGET, and ASCERTAIN), focusing on the recommended sarilumab dose of 200 mg.
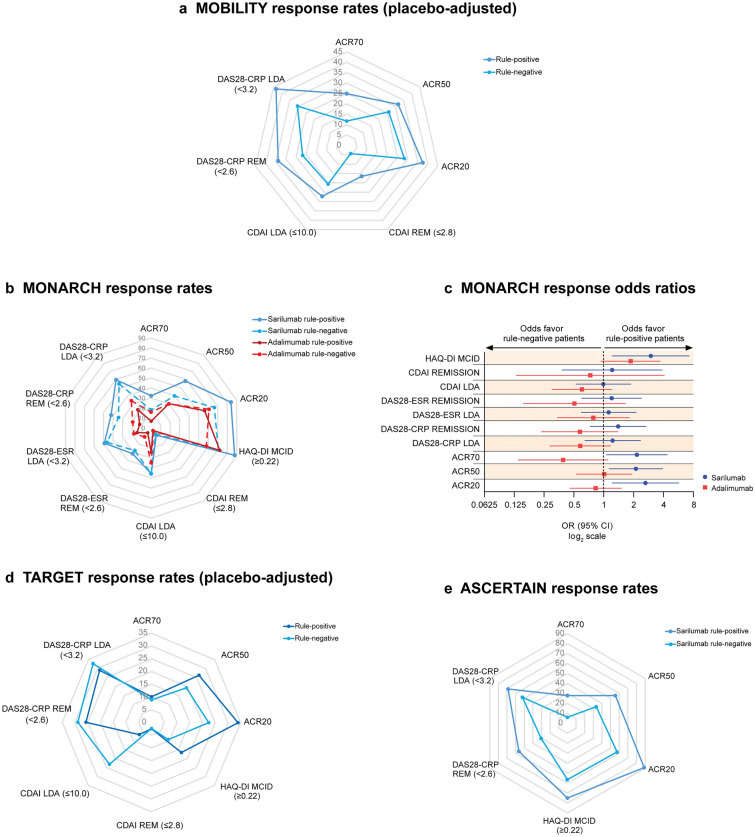
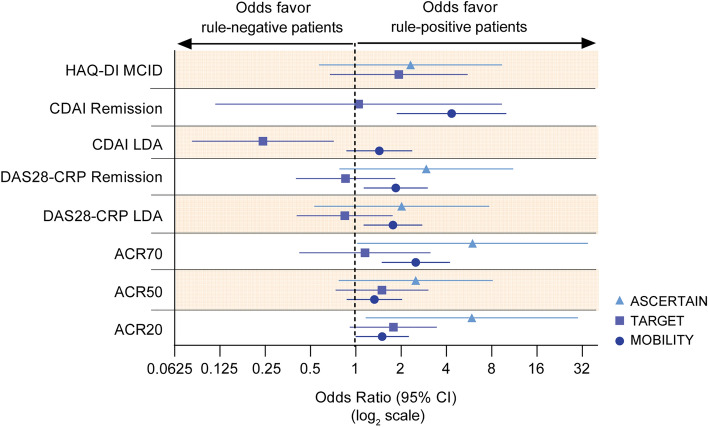
Results: In the training set, the presence of anti-cyclic citrullinated peptide antibodies, combined with C-reactive protein > 12.3 mg/l, was identified as the "rule" that predicts American College of Rheumatology 20% response (ACR20) to sarilumab. In testing, the rule reliably predicted response to sarilumab in MOBILITY, MONARCH, and ASCERTAIN for many efficacy parameters (e.g., ACR70 and the 28-joint disease activity score using CRP [DAS28-CRP] remission). The rule applied less to TARGET, which recruited individuals refractory to tumor necrosis factor inhibitors. The potential clinical benefit of the rule was highlighted in a clinical scenario based on MONARCH data, which found that increased ACR70 rates could be achieved by treating either rule-positive patients with sarilumab or rule-negative patients with adalimumab.
Conclusions: Well-established and clinically feasible blood biomarkers can guide individual treatment choice. Real-world validation of the rule identified in this post hoc analysis is merited.
Clinical trial registration: NCT01061736, NCT02332590, NCT01709578, NCT01768572.
Keywords: Adalimumab; Clinical trial; Machine learning; Precision medicine; Rheumatoid arthritis; Sarilumab.
© 2021. The Author(s).
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
