

Socioeconomic inequalities in prevalence and development of multimorbidity across adulthood: A longitudinal analysis of the MRC 1946 National Survey of Health and Development in the UK
- PMID: 34520470
- PMCID: PMC8601600
- DOI: 10.1371/journal.pmed.1003775
Socioeconomic inequalities in prevalence and development of multimorbidity across adulthood: A longitudinal analysis of the MRC 1946 National Survey of Health and Development in the UK
Abstract
Background: We aimed to estimate multimorbidity trajectories and quantify socioeconomic inequalities based on childhood and adulthood socioeconomic position (SEP) in the risks and rates of multimorbidity accumulation across adulthood.
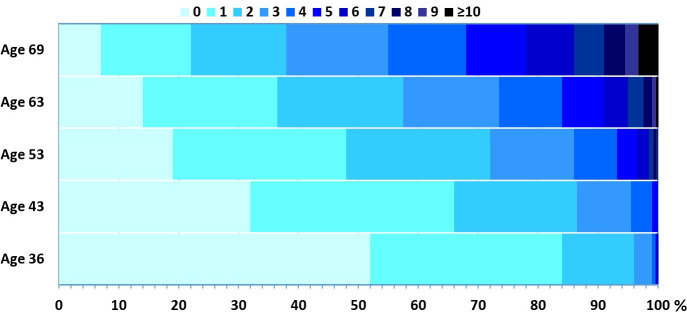
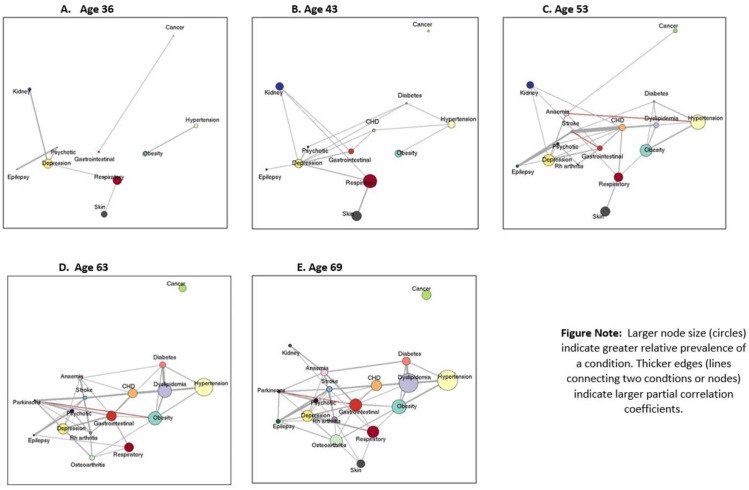
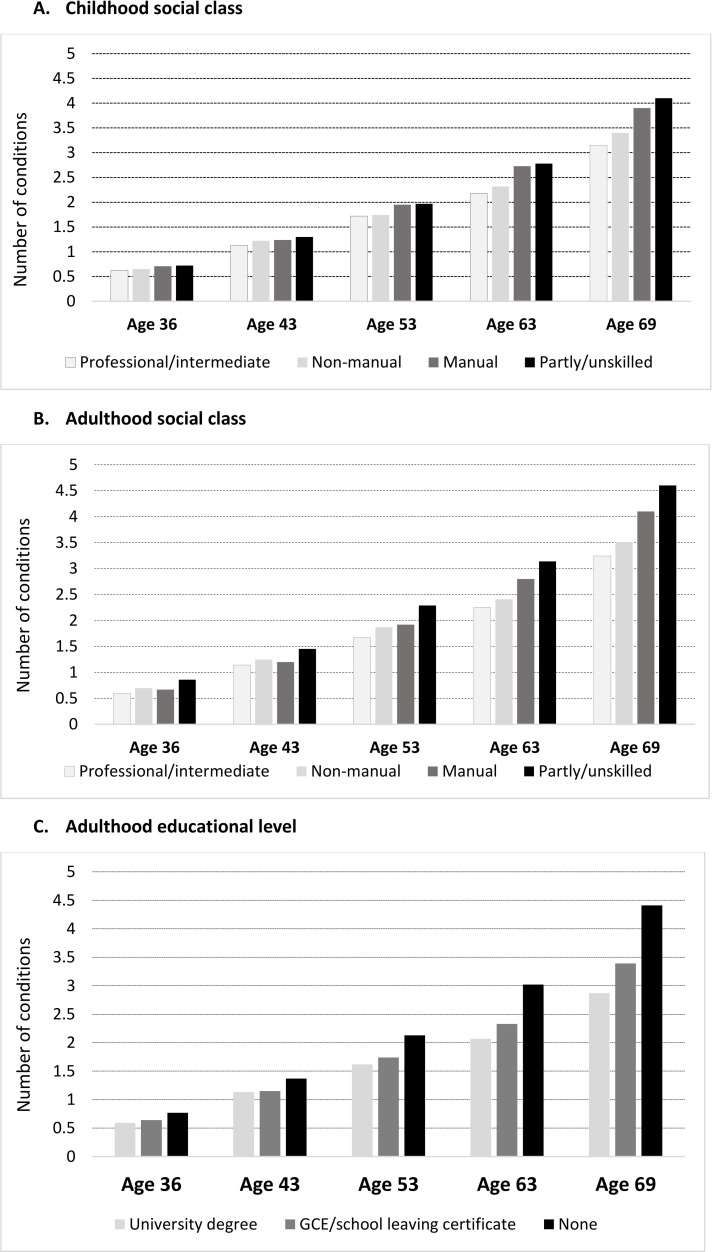
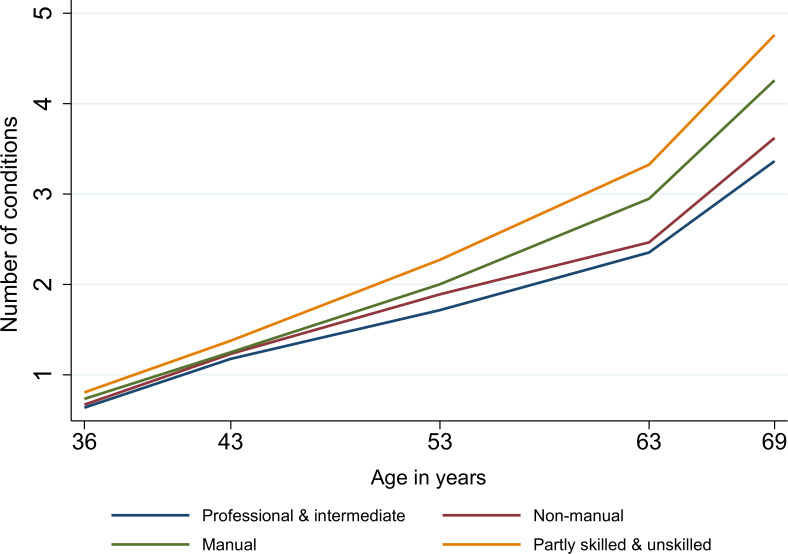
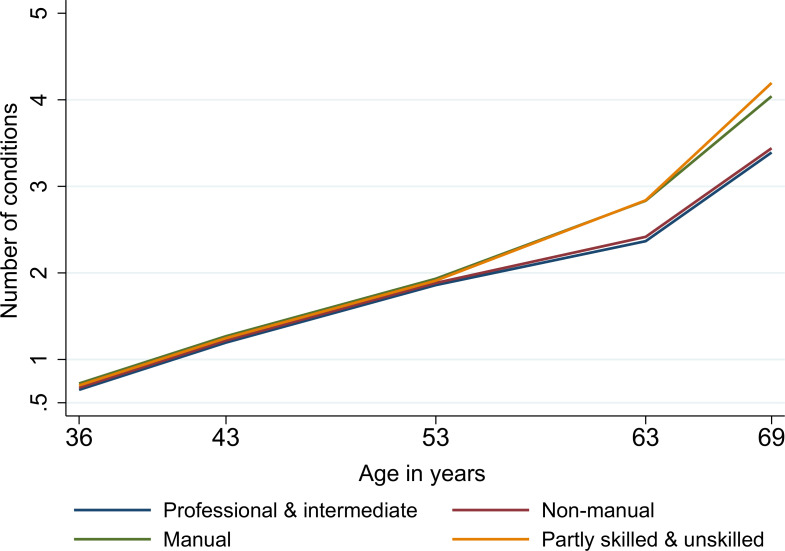
Methods and findings: Participants from the UK 1946 National Survey of Health and Development (NSHD) birth cohort study who attended the age 36 years assessment in 1982 and any one of the follow-up assessments at ages 43, 53, 63, and 69 years (N = 3,723, 51% males). Information on 18 health conditions was based on a combination of self-report, biomarkers, health records, and prescribed medications. We estimated multimorbidity trajectories and delineated socioeconomic inequalities (based on childhood and adulthood social class and highest education) in multimorbidity at each age and in longitudinal trajectories. Multimorbidity increased with age (0.7 conditions at 36 years to 3.7 at 69 years). Multimorbidity accumulation was nonlinear, accelerating with age at the rate of 0.08 conditions/year (95% CI 0.07 to 0.09, p < 0.001) at 36 to 43 years to 0.19 conditions/year (95% CI 0.18 to 0.20, p < 0.001) at 63 to 69 years. At all ages, the most socioeconomically disadvantaged had 1.2 to 1.4 times greater number of conditions on average compared to the most advantaged. The most disadvantaged by each socioeconomic indicator experienced an additional 0.39 conditions (childhood social class), 0.83 (adult social class), and 1.08 conditions (adult education) at age 69 years, independent of all other socioeconomic indicators. Adverse adulthood SEP was associated with more rapid accumulation of multimorbidity, resulting in 0.49 excess conditions in partly/unskilled compared to professional/intermediate individuals between 63 and 69 years. Disadvantaged childhood social class, independently of adulthood SEP, was associated with accelerated multimorbidity trajectories from age 53 years onwards. Study limitations include that the NSHD cohort is composed of individuals of white European heritage only, and findings may not be generalizable to the non-white British population of the same generation and did not account for other important dimensions of SEP such as income and wealth.
Conclusions: In this study, we found that socioeconomically disadvantaged individuals have earlier onset and more rapid accumulation of multimorbidity resulting in widening inequalities into old age, with independent contributions from both childhood and adulthood SEP.
Conflict of interest statement
I have read the journal’s policy and the following authors of this manuscript have competing interests: NC is remunerated for her membership of a data safety and monitoring committee of a trial sponsored by AstraZeneca. The remaining authors have no competing interests to declare. All other authors have declared that no competing interests exist.
Figures
References
-
- Academy of Medical Sciences. Multimorbidity: a priority for global research. April, 2018. 2018.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
