

Outcomes of Participants With Diabetes in the ISCHEMIA Trials
- PMID: 34521217
- PMCID: PMC8545918
- DOI: 10.1161/CIRCULATIONAHA.121.054439
Outcomes of Participants With Diabetes in the ISCHEMIA Trials
Abstract
Background: Among patients with diabetes and chronic coronary disease, it is unclear if invasive management improves outcomes when added to medical therapy.
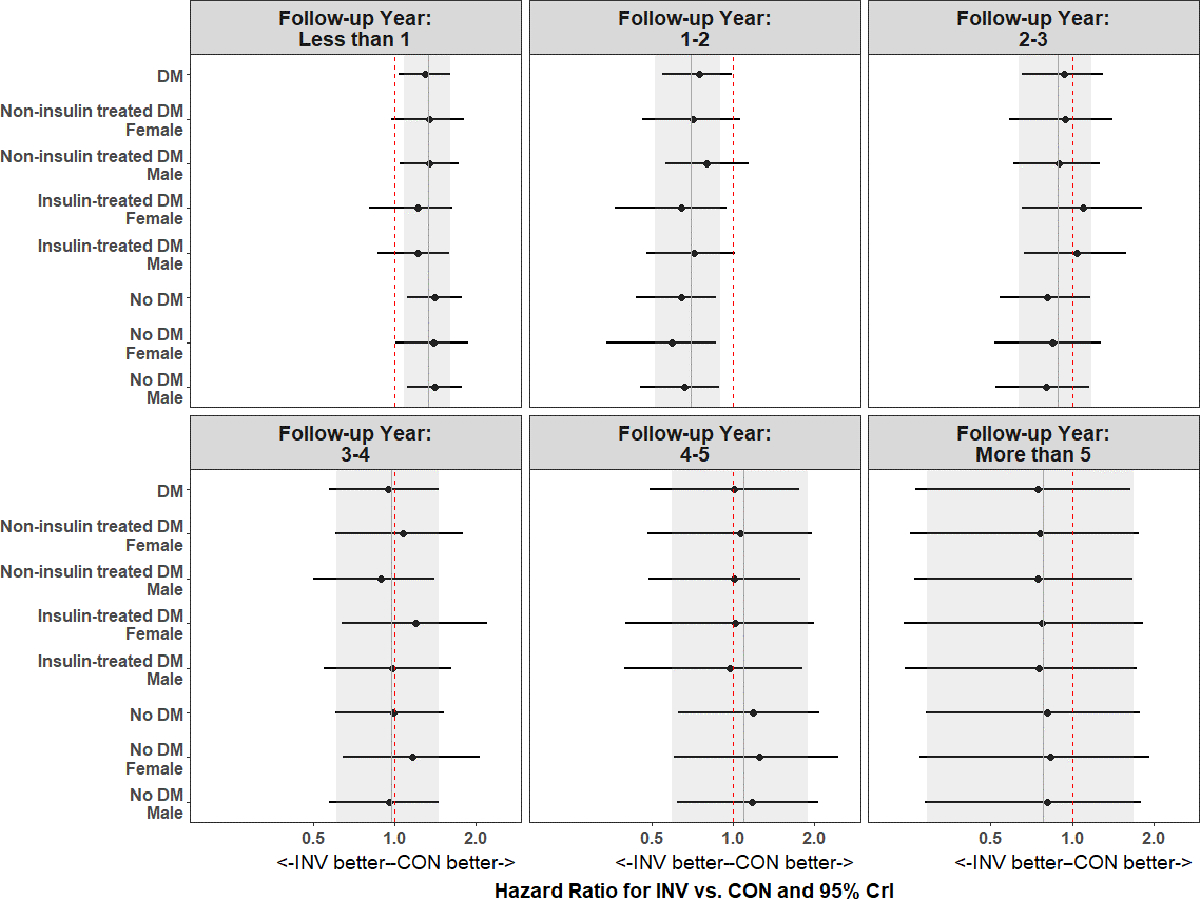
Methods: The ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trials (ie, ISCHEMIA and ISCHEMIA-Chronic Kidney Disease) randomized chronic coronary disease patients to an invasive (medical therapy + angiography and revascularization if feasible) or a conservative approach (medical therapy alone with revascularization if medical therapy failed). Cohorts were combined after no trial-specific effects were observed. Diabetes was defined by history, hemoglobin A1c ≥6.5%, or use of glucose-lowering medication. The primary outcome was all-cause death or myocardial infarction (MI). Heterogeneity of effect of invasive management on death or MI was evaluated using a Bayesian approach to protect against random high or low estimates of treatment effect for patients with versus without diabetes and for diabetes subgroups of clinical (female sex and insulin use) and anatomic features (coronary artery disease severity or left ventricular function).
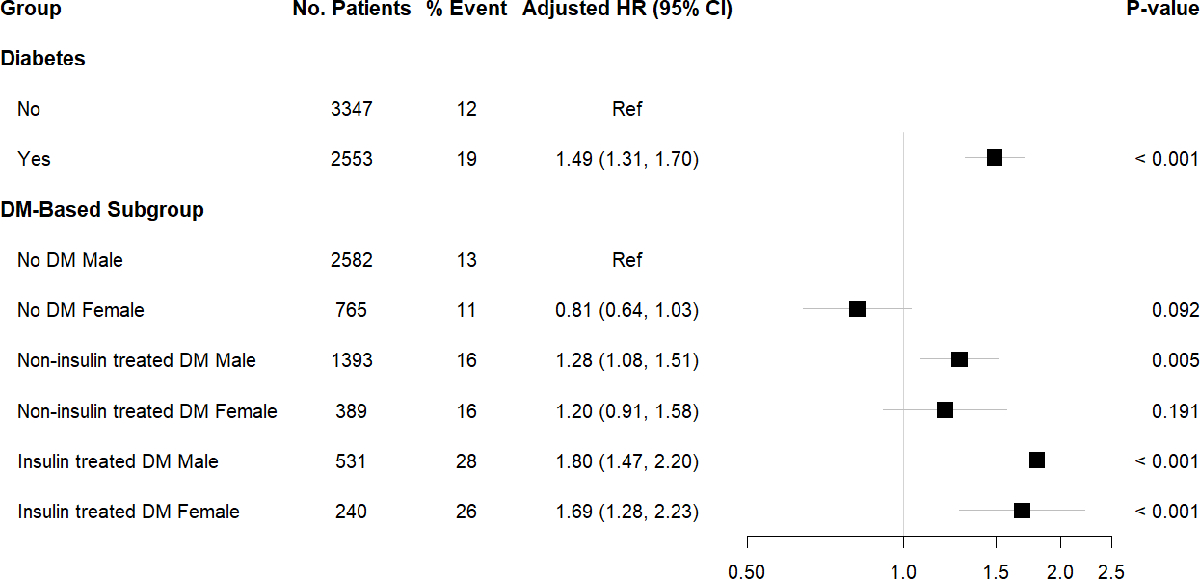
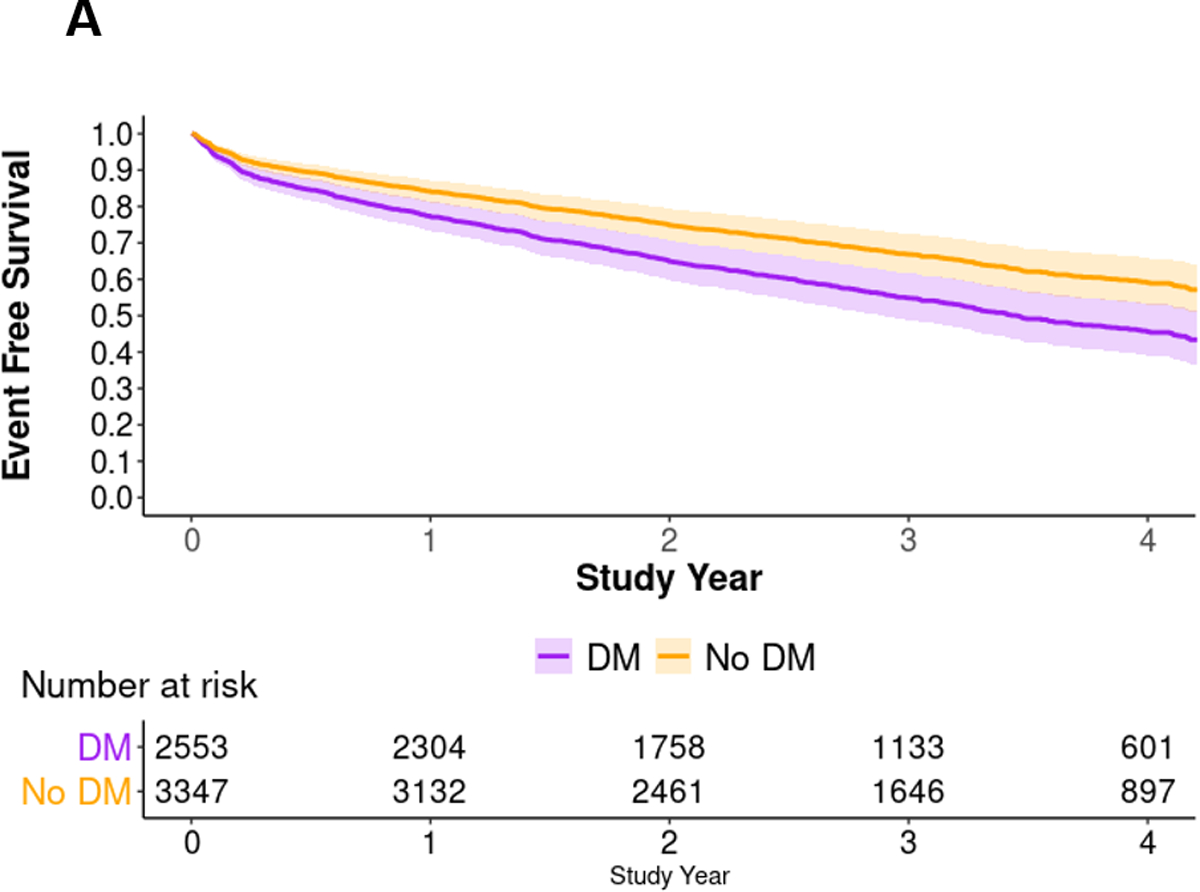
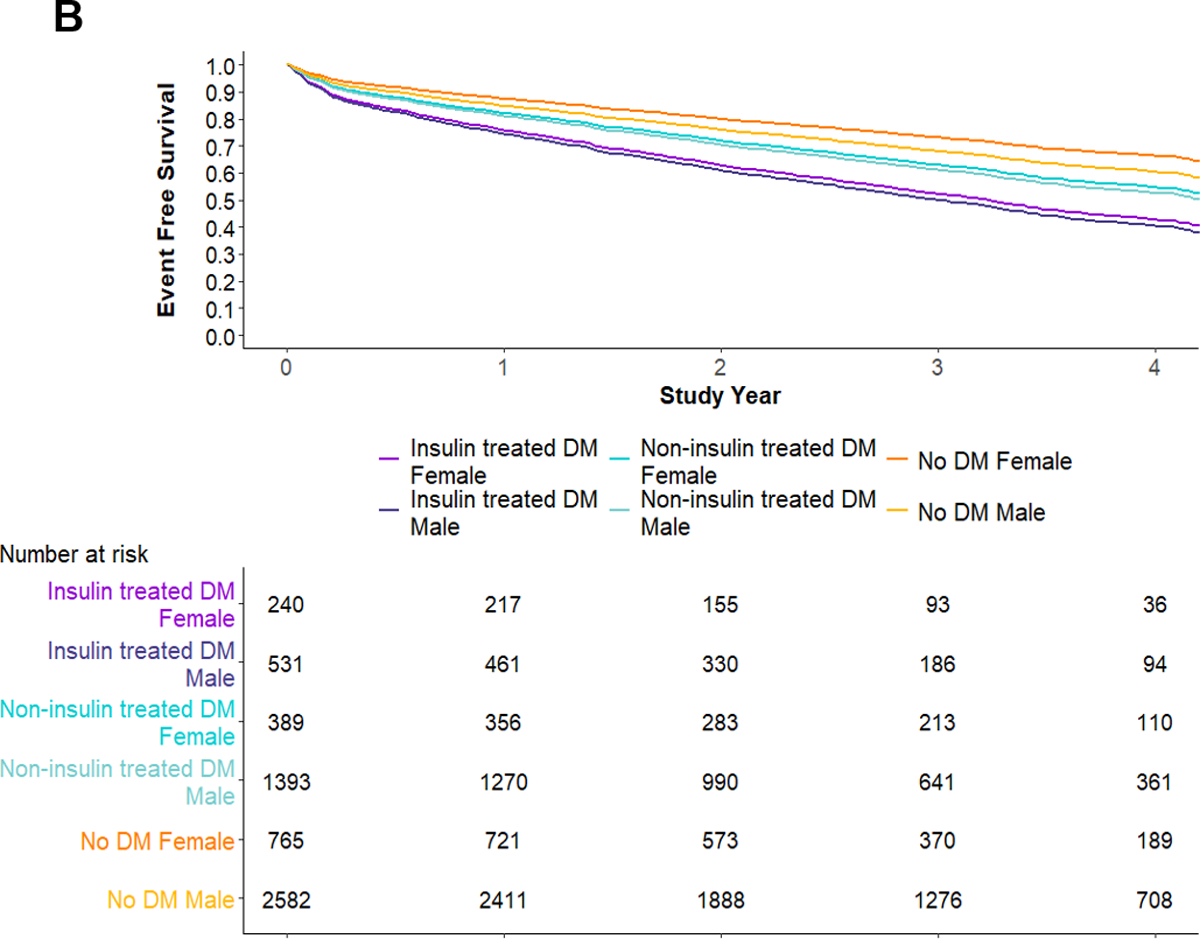
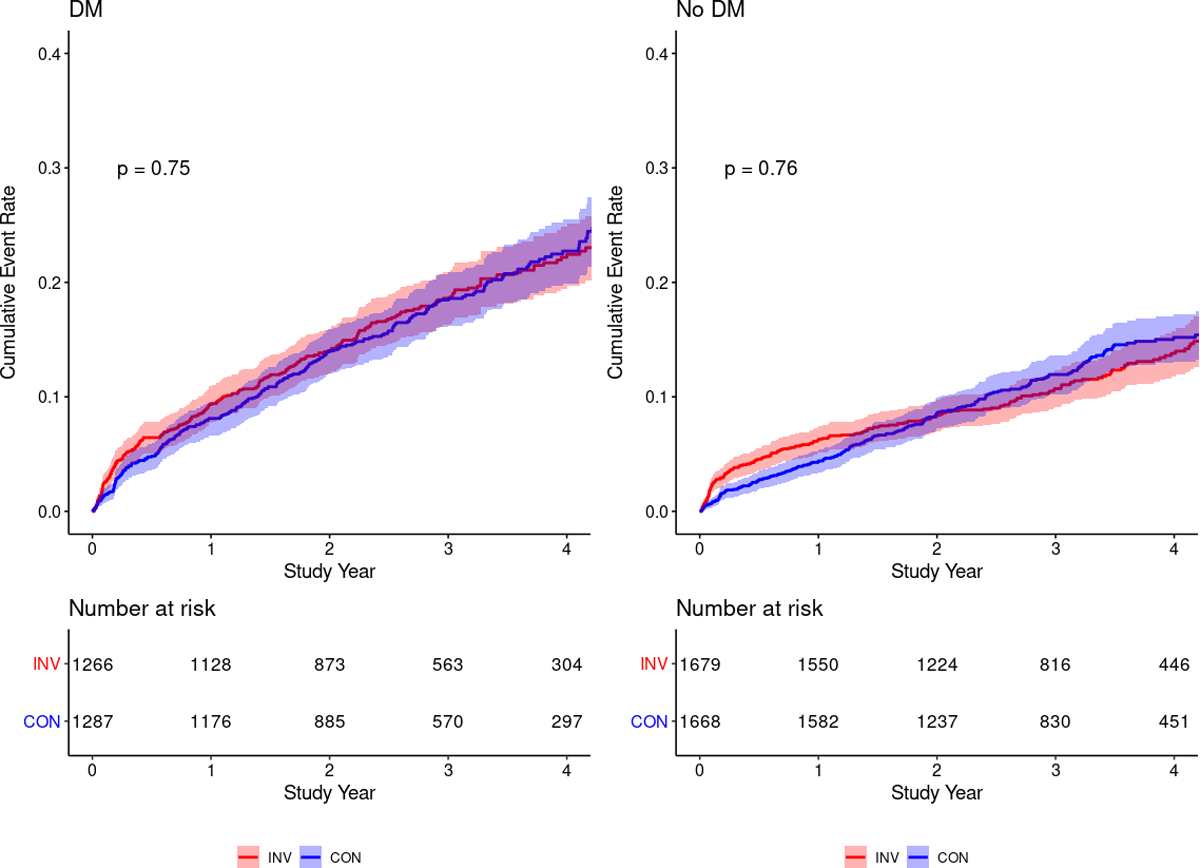
Results: Of 5900 participants with complete baseline data, the median age was 64 years (interquartile range, 57-70), 24% were female, and the median estimated glomerular filtration was 80 mL·min-1·1.73-2 (interquartile range, 64-95). Among the 2553 (43%) of participants with diabetes, the median percent hemoglobin A1c was 7% (interquartile range, 7-8), and 30% were insulin-treated. Participants with diabetes had a 49% increased hazard of death or MI (hazard ratio, 1.49 [95% CI, 1.31-1.70]; P<0.001). At median 3.1-year follow-up the adjusted event-free survival was 0.54 (95% bootstrapped CI, 0.48-0.60) and 0.66 (95% bootstrapped CI, 0.61-0.71) for patients with diabetes versus without diabetes, respectively, with a 12% (95% bootstrapped CI, 4%-20%) absolute decrease in event-free survival among participants with diabetes. Female and male patients with insulin-treated diabetes had an adjusted event-free survival of 0.52 (95% bootstrapped CI, 0.42-0.56) and 0.49 (95% bootstrapped CI, 0.42-0.56), respectively. There was no difference in death or MI between strategies for patients with diabetes versus without diabetes, or for clinical (female sex or insulin use) or anatomic features (coronary artery disease severity or left ventricular function) of patients with diabetes.
Conclusions: Despite higher risk for death or MI, chronic coronary disease patients with diabetes did not derive incremental benefit from routine invasive management compared with initial medical therapy alone. Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT01471522.
Keywords: Bayes theorem; coronary artery disease; diabetes mellitus; insulin; progression-free survival; renal insufficiency, chronic; ventricular function, left.
Figures
References
-
- Cavender MA, Steg PG, Smith SC, Eagle K, Ohman EM, Goto S, Kuder J, Im K, Wilson PWF, Bhatt DL, et al. Impact of Diabetes Mellitus on Hospitalization for Heart Failure, Cardiovascular Events, and Death. Circulation 2015;132:923–931. - PubMed
-
- Arnold Suzanne V, Bhatt Deepak L, Barsness Gregory W, Beatty Alexis L, Deedwania Prakash C, Inzucchi Silvio E, Kosiborod Mikhail, Leiter Lawrence A., Lipska Kasia J., Newman Jonathan D., et al. Clinical Management of Stable Coronary Artery Disease in Patients With Type 2 Diabetes Mellitus: A Scientific Statement From the American Heart Association. Circulation 2020;141:e779–e806. - PubMed
-
- Boden WE, O’Rourke RA, Teo KK, Hartigan PM, Maron DJ, Kostuk WJ, Knudtson M, Dada M, Casperson P, Harris CL, et al. Optimal Medical Therapy with or without PCI for Stable Coronary Disease. New England Journal of Medicine 2007;356:1503–1516. - PubMed
-
- Farkouh ME, Domanski M, Sleeper LA, Siami FS, Dangas G, Mack M, Yang M, Cohen DJ, Rosenberg Y, Solomon SD, et al. Strategies for Multivessel Revascularization in Patients with Diabetes. New England Journal of Medicine 2012;367:2375–2384. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
