

Clinical characteristics and risk factors of fatal patients with COVID-19: a retrospective cohort study in Wuhan, China
- PMID: 34521370
- PMCID: PMC8439538
- DOI: 10.1186/s12879-021-06585-8
Clinical characteristics and risk factors of fatal patients with COVID-19: a retrospective cohort study in Wuhan, China
Abstract
Background: The coronavirus disease 2019 (COVID-19) has caused a global pandemic, resulting in considerable mortality. The risk factors, clinical treatments, especially comprehensive risk models for COVID-19 death are urgently warranted.
Methods: In this retrospective study, 281 non-survivors and 712 survivors with propensity score matching by age, sex, and comorbidities were enrolled from January 13, 2020 to March 31, 2020.
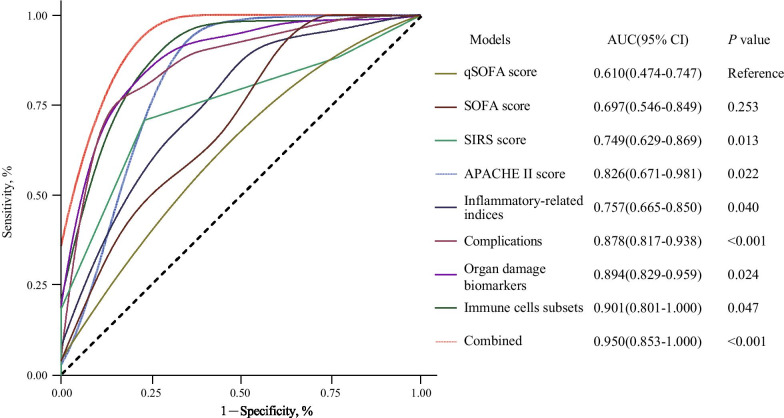
Results: Higher SOFA, qSOFA, APACHE II and SIRS scores, hypoxia, elevated inflammatory cytokines, multi-organ dysfunction, decreased immune cell subsets, and complications were significantly associated with the higher COVID-19 death risk. In addition to traditional predictors for death risk, including APACHE II (AUC = 0.83), SIRS (AUC = 0.75), SOFA (AUC = 0.70) and qSOFA scores (AUC = 0.61), another four prediction models that included immune cells subsets (AUC = 0.90), multiple organ damage biomarkers (AUC = 0.89), complications (AUC = 0.88) and inflammatory-related indexes (AUC = 0.75) were established. Additionally, the predictive accuracy of combining these risk factors (AUC = 0.950) was also significantly higher than that of each risk group alone, which was significant for early clinical management for COVID-19.
Conclusions: The potential risk factors could help to predict the clinical prognosis of COVID-19 patients at an early stage. The combined model might be more suitable for the death risk evaluation of COVID-19.
Keywords: COVID-19; Death risk; Immune cells subsets; Risk prediction models.
© 2021. The Author(s).
Conflict of interest statement
We declare that we have no conflicts of interest.
Figures
References
-
- World Health Organization. Coronavirus disease (COVID-19) outbreak situation. https://www.who.int/emergencies/diseases/novel-coronavirus-2019. Accessed 5 Jan 2020
-
- American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med 1992; 20(6):864–74. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
