

Cholbam® and Zellweger spectrum disorders: treatment implementation and management
- PMID: 34521419
- PMCID: PMC8439061
- DOI: 10.1186/s13023-021-01940-z
Cholbam® and Zellweger spectrum disorders: treatment implementation and management
Abstract
Background: Zellweger spectrum disorders (ZSDs) are a rare, heterogenous group of autosomal recessively inherited disorders characterized by reduced peroxisomes numbers, impaired peroxisomal formation, and/or defective peroxisomal functioning. In the absence of functional peroxisomes, bile acid synthesis is disrupted, and multisystem disease ensues with abnormalities in the brain, liver, kidneys, muscle, eyes, ears, and nervous system.
Main body: Liver disease may play an important role in morbidity and mortality, with hepatic fibrosis that can develop as early as the postnatal period and often progressing to cirrhosis within the first year of life. Because hepatic dysfunction can have numerous secondary effects on other organ systems, thereby impacting the overall disease severity, the treatment of liver disease in patients with ZSD is an important focus of disease management. Cholbam® (cholic acid), approved by the U.S. Food and Drug Administration in March 2015, is currently the only therapy approved as adjunctive treatment for patients with ZSDs and single enzyme bile acid synthesis disorders. This review will focus on the use of CA therapy in the treatment of liver disease associated with ZSDs, including recommendations for initiating and maintaining CA therapy and the limitations of available clinical data supporting its use in this patient population.
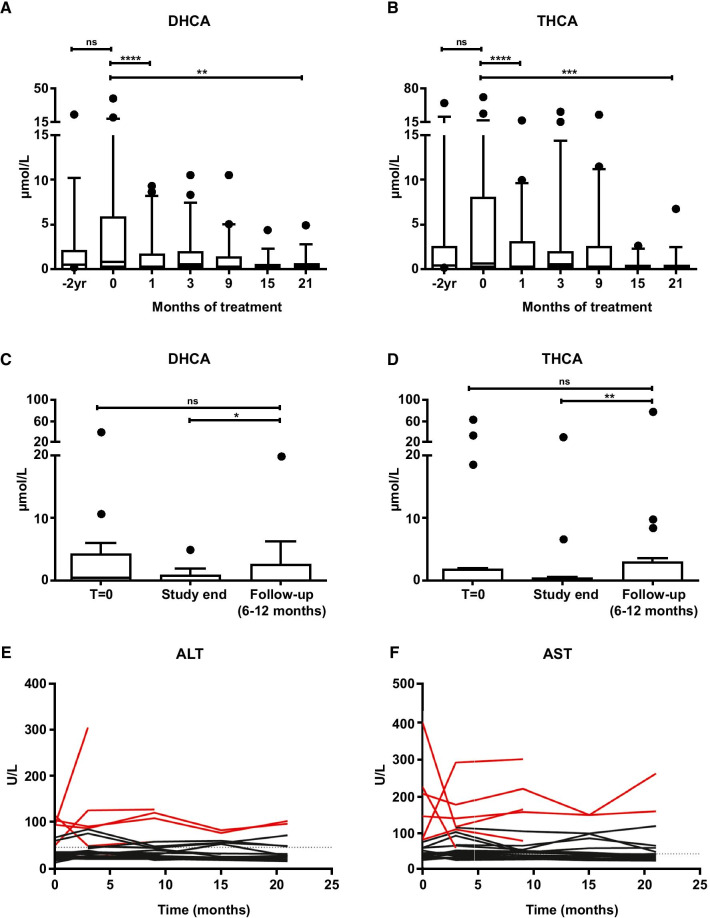
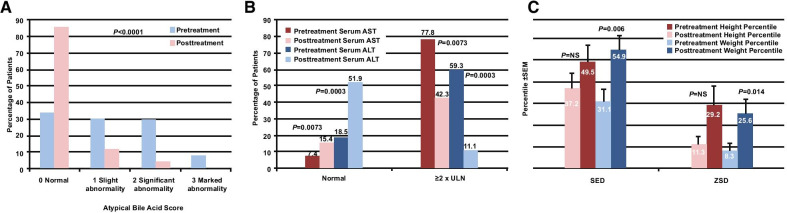
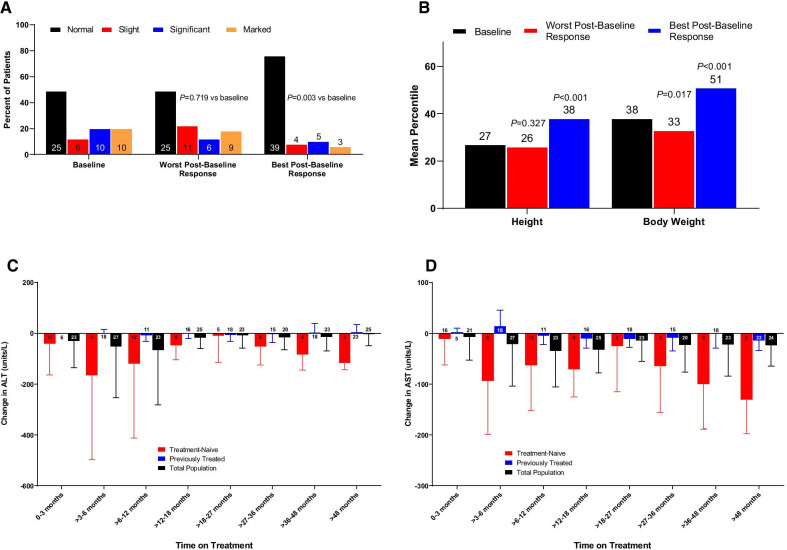
Conclusions: Cholbam is a safe and well-tolerated treatment for patients with ZSDs that has been shown to improve liver chemistries and reduce toxic bile acid intermediates in the majority of patients with ZSD. Due to the systemic impacts of hepatic damage, Cholbam should be initiated in patients without signs of advanced liver disease.
Keywords: Cholic acid therapy; Hepatic injury; Peroxisome biogenesis disorder; Zellweger disease; Zellweger spectrum disorder.
© 2021. The Author(s).
Conflict of interest statement
JN: Consulting for Travere Therapeutics. ZA: Consulting and speaking for Travere Therapeutics (2018–2019); advisory board for BioMarin (2018) and Travere Therapeutics (2017). YE: Consulting for Travere Therapeutics. EH: Consulting for Travere Therapeutics. JH: Equity interest in Asklepion; consulting for Alnylam, FrieslandCampina, Travere Therapeutics, Mirum, and Albireo. RH: Consulting and speaking for Alexion and Travere Therapeutics. SP: Consulting for Travere Therapeutics.
Figures

References
-
- National Organization for Rare Disorders. Zellweger spectrum disorders. 2016. https://rarediseases.org/rare-diseases/zellweger-spectrum-disorders/. Accessed 15 Mar 2021.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
