

When neurologists diagnose functional neurological disorder, why don't they code for it?
- PMID: 34521502
- PMCID: PMC8920954
- DOI: 10.1017/S1092852921000833
When neurologists diagnose functional neurological disorder, why don't they code for it?
Abstract
Objective:: Clinicians who recognize functional neurological disorders (FND) may not share that diagnosis with patients. Poor communication delays treatment and contributes to substantial disability in FND. Diagnostic (ICD-10) coding, one form of medical communication, offers an insight into clinicians’ face-to-face communication. Therefore, quantifying the phenomenon of non-coding, and identifying beliefs and practice habits that reduce coding, may suggest routes to improve medical communication in FND.
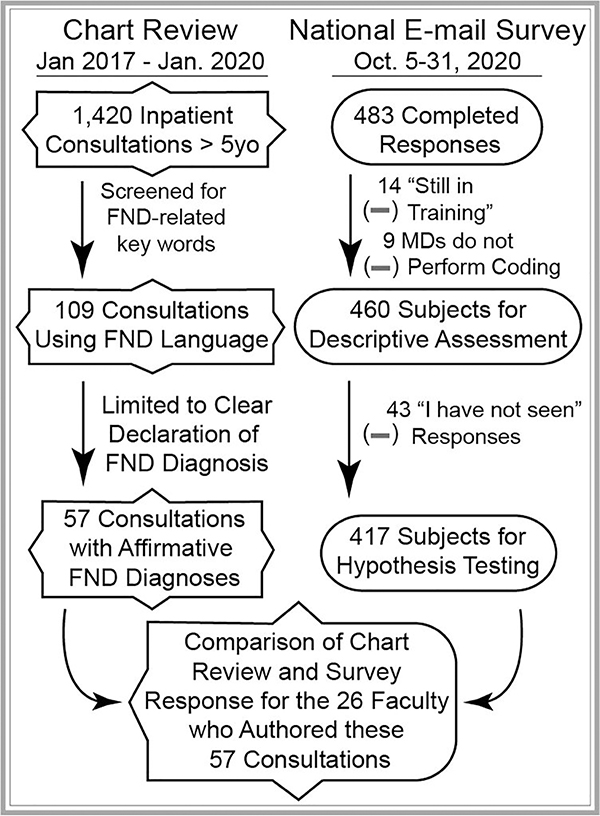
Methods:: We reviewed all pediatric neurology consultations in our hospital from 2017–2020, selecting those in which neurologists explicitly stated an FND-related diagnosis (N=57). We identified the neurological symptoms and ICD-10 codes assigned for each consultation. In parallel, we reviewed all encounters that utilized FND-related codes to determine whether insurers paid for this care. Finally, we assessed beliefs and practices that influence FND-related coding through a nationwide survey of pediatric neurologists (N=460).
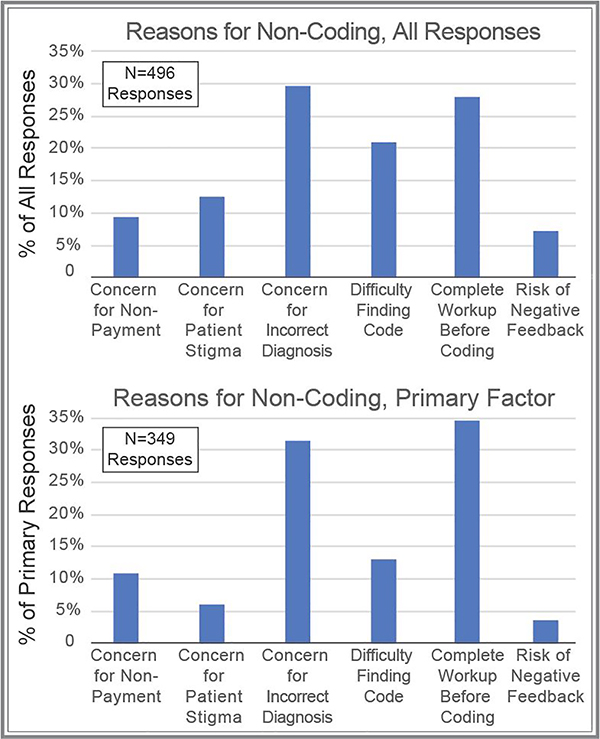
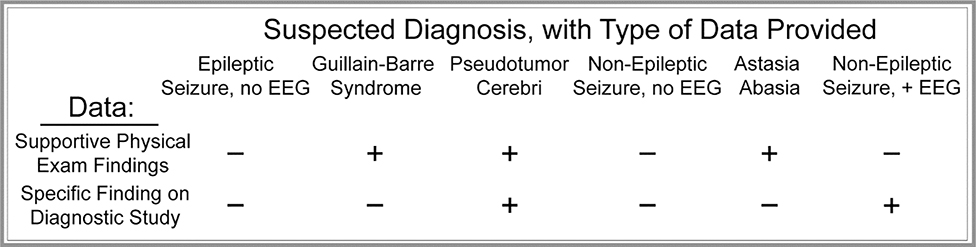
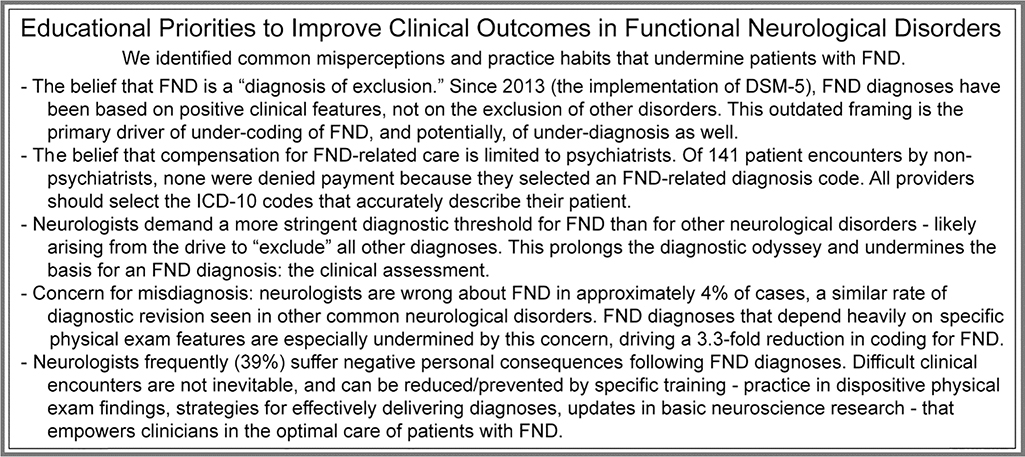
Results:: After diagnosing FND, neurologists selected FND-related ICD-10 codes in only 22.8% of consultations. 96.2% of neurologists estimated that they would code for non-epileptic seizure (NES) when substantiated by EEG; in practice, they coded for 36.7% of such consultations. For other FND manifestations, neurologists coded in only 13.3% of cases. When presented with FND and non-FND scenarios with equal levels of information, neurologists coded for FND 41% less often. The strongest predictor of non-coding was the outdated belief that FND is a diagnosis of exclusion. Coding for FND never resulted in insurance non-payment.
Conclusion:: Non-coding for FND is common. Most factors that amplify non-coding also hinder face-to-face communication. Research based on ICD-10 coding (e.g., prevalence, cost) may underestimate the impact of FND by >4-fold.
Figures
References
-
- Stone J, Carson A, Duncan R, et al. Who is referred to neurology clinics?--the diagnoses made in 3781 new patients. Clinical neurology and neurosurgery. 2010;112(9):747–751. - PubMed
-
- Gelauff J, Stone J. Prognosis of functional neurologic disorders. Handb Clin Neurol. 2016;139:523–541. - PubMed
-
- Carson A, Stone J, Hibberd C, et al. Disability, distress and unemployment in neurology outpatients with symptoms ‘unexplained by organic disease’. J Neurol Neurosurg Psychiatry. 2011;82(7):810–813. - PubMed
-
- Stone J Functional neurological disorders: the neurological assessment as treatment. Pract Neurol. 2016;16(1):7–17. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
