

Wall eyed bilateral internuclear ophthalmoplegia (WEBINO) syndrome as a false localising sign in intracranial haemorrhage due to snake bite
- PMID: 34521743
- PMCID: PMC8442054
- DOI: 10.1136/bcr-2021-244830
Wall eyed bilateral internuclear ophthalmoplegia (WEBINO) syndrome as a false localising sign in intracranial haemorrhage due to snake bite
Abstract
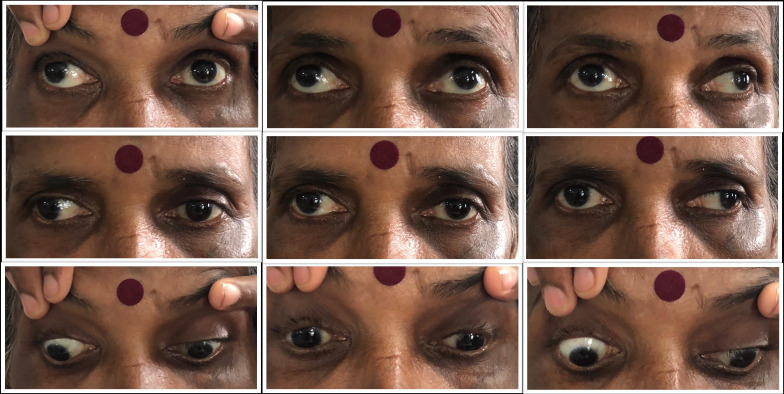
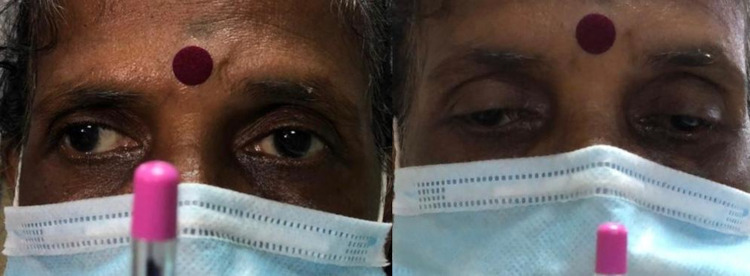
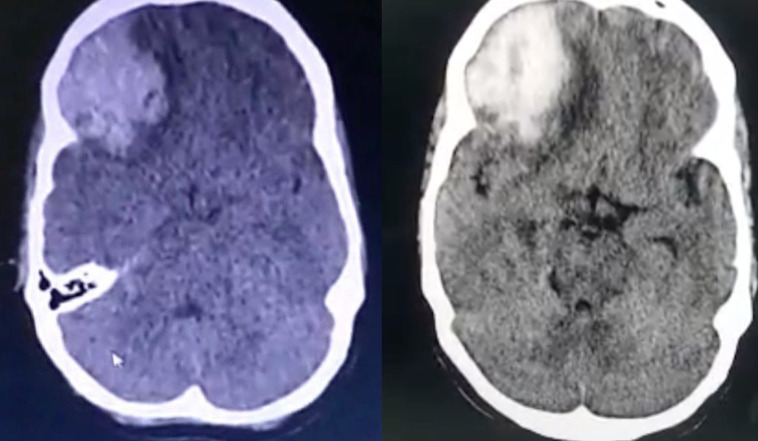
A 48-year-old woman presented with sudden-onset altered sensorium 2 days after a snake bite (unidentified species) and was found to have a large right frontal intracerebral haemorrhage (ICH) with transtentorial herniation (TTH) causing brain stem compression. A day later, neurological examination revealed internuclear ophthalmoplegia (INO) fitting the clinical description of wall eyed bilateral INO syndrome. INO is a rare ocular motor sign, the most common causes being brain stem infarction, haemorrhage or demyelinating disease. It rarely acts as a false localising sign, such as in this case, and in an even rarer cause for ICH, that is, haemotoxic snake bite without initial evidence of coagulopathy. An emphasis needs to be laid on detailed physical examination, often considered a lost art nowadays, to help detect subtle clinical signs which could herald ominous complications of conditions like TTH and help in early diagnosis and treatment of the same.
Keywords: brain stem / cerebellum; cranial nerves; emergency medicine; neurology.
© BMJ Publishing Group Limited 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- McGettrick P, Eustace P. The w.e.b.i.n.o. syndrome. Neuroophthalmology 1985;5:109–15. 10.3109/01658108509014426 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical