

Changes in muscle ultrasound for the diagnosis of intensive care unit acquired weakness in critically ill patients
- PMID: 34521934
- PMCID: PMC8440559
- DOI: 10.1038/s41598-021-97680-y
Changes in muscle ultrasound for the diagnosis of intensive care unit acquired weakness in critically ill patients
Abstract
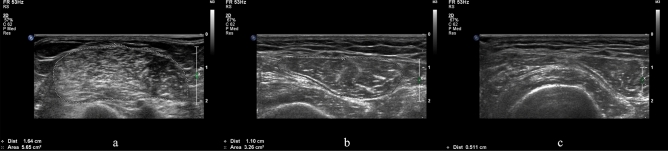
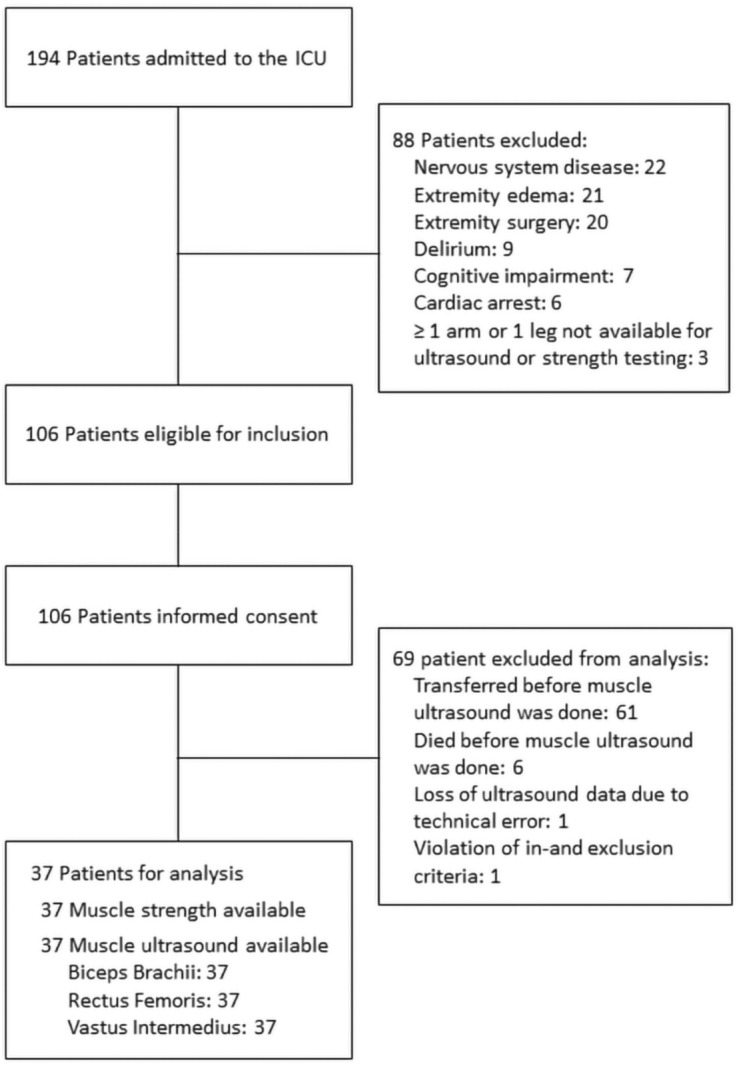
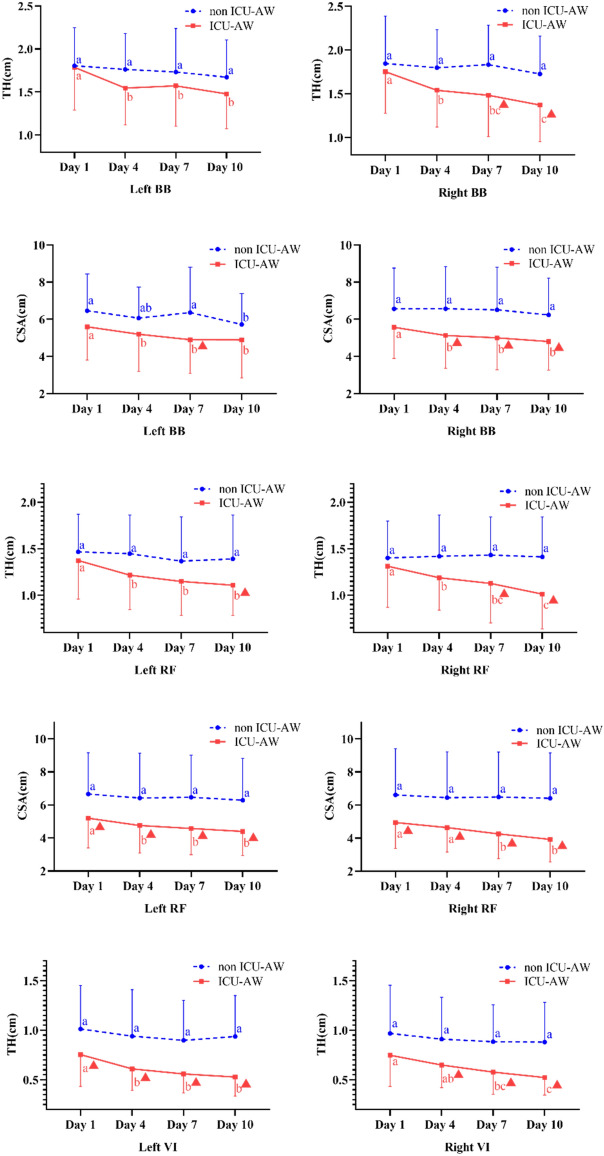
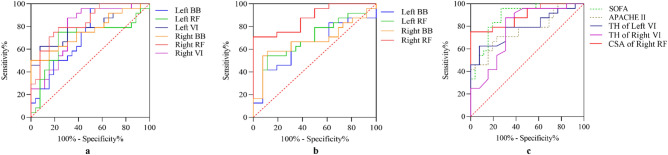
To test diagnostic accuracy of changes in thickness (TH) and cross-sectional area (CSA) of muscle ultrasound for diagnosis of intensive care unit acquired weakness (ICU-AW). Fully conscious patients were subjected to muscle ultrasonography including measuring the changes in TH and CSA of biceps brachii (BB) muscle, vastus intermedius (VI) muscle, and rectus femoris (RF) muscles over time. 37 patients underwent muscle ultrasonography on admission day, day 4, day 7, and day 10 after ICU admission, Among them, 24 were found to have ICW-AW. Changes in muscle TH and CSA of RF muscle on the right side showed remarkably higher ROC-AUC and the range was from 0.734 to 0.888. Changes in the TH of VI muscle had fair ROC-AUC values which were 0.785 on the left side and 0.779 on the right side on the 10th day after ICU admission. Additionally, Sequential Organ Failure Assessment (SOFA), Acute Physiology, and Chronic Health Evaluation II (APACHE II) scores also showed good discriminative power on the day of admission (ROC-AUC 0.886 and 0.767, respectively). Ultrasonography of changes in muscles, especially in the TH of VI muscle on both sides and CSA of RF muscle on the right side, presented good diagnostic accuracy. However, SOFA and APACHE II scores are better options for early ICU-AW prediction due to their simplicity and time efficiency.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
