

Stratifying the risk of NAFLD in patients with HIV under combination antiretroviral therapy (cART)
- PMID: 34522873
- PMCID: PMC8427211
- DOI: 10.1016/j.eclinm.2021.101116
Stratifying the risk of NAFLD in patients with HIV under combination antiretroviral therapy (cART)
Abstract
Background: De novo steatosis is the main criteria for non-alcoholic fatty liver disease (NAFLD), which is becoming a clinically relevant comorbidity in HIV-infected patients. This may be due to the HIV virus itself, as well as long-term toxicities deriving from antiretroviral therapy. Therefore, HIV infected patients require prevention and monitoring regarding NAFLD.
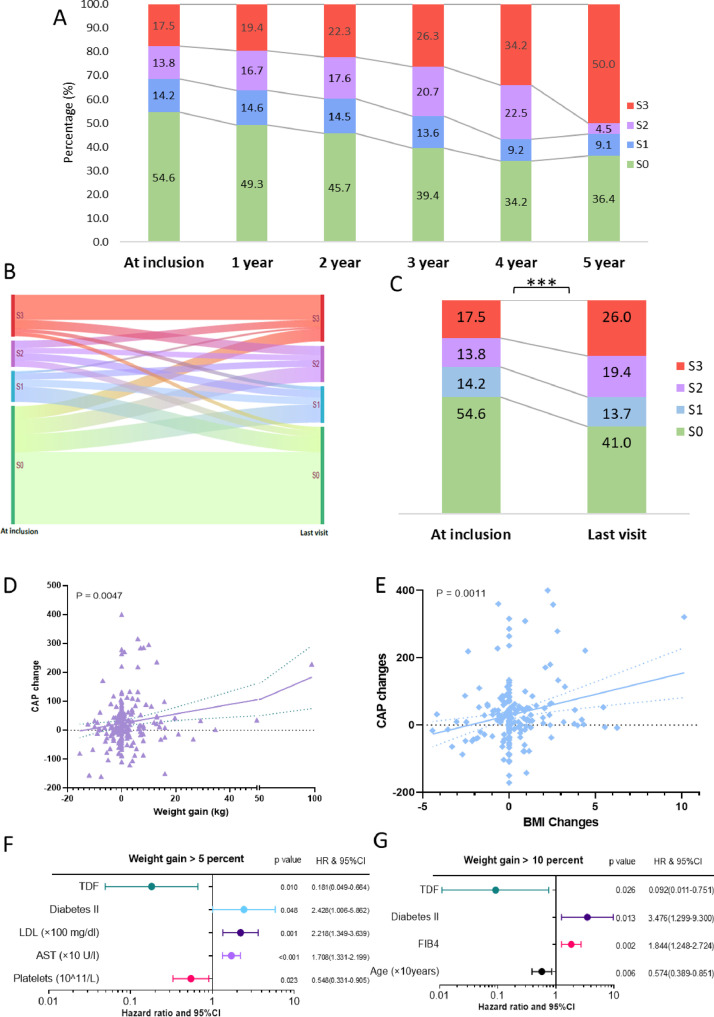
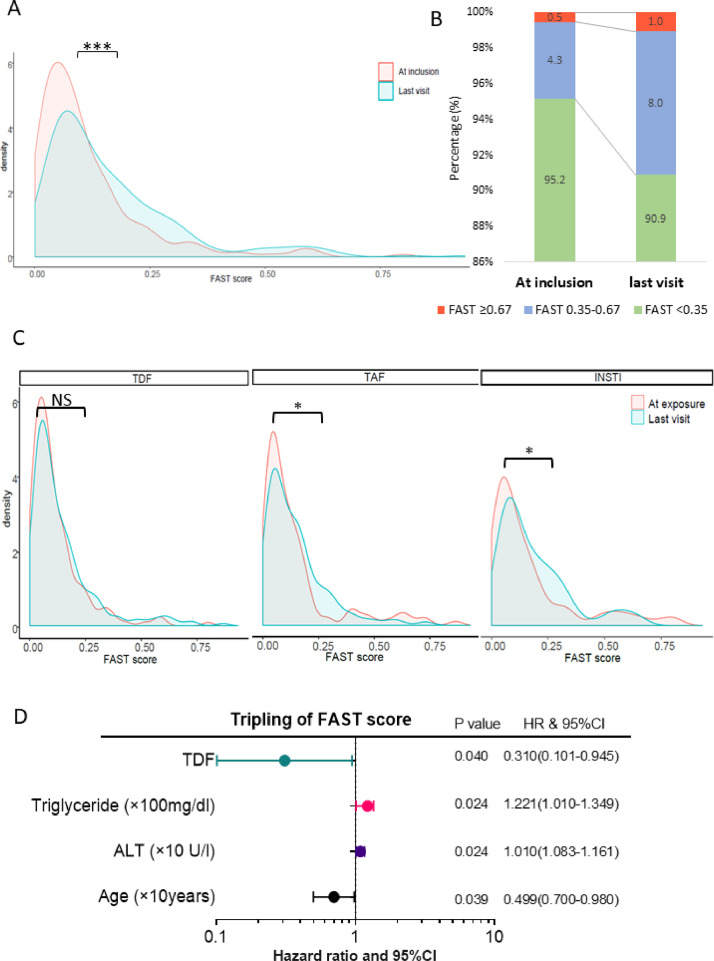
Methods: This study investigated the differential role of body mass index (BMI) and combination antiretroviral treatment (cART) drugs on NAFLD progression. This single center prospective longitudinal observational study enrolled HIV monoinfected individuals between August 2013 to December 2018 with yearly visits. Each visit included liver stiffness and steatosis [defined as controlled attenuation parameter (CAP)>237 dB/m] assessment by annually transient elastography using an M- or XL-probe of FibroScan, and calculation of the novel FibroScan-AST (FAST) score. Risk factors for denovo/progressed steatosis and tripling of FAST-score increase were investigated using Cox regression model with time-dependent covariates.
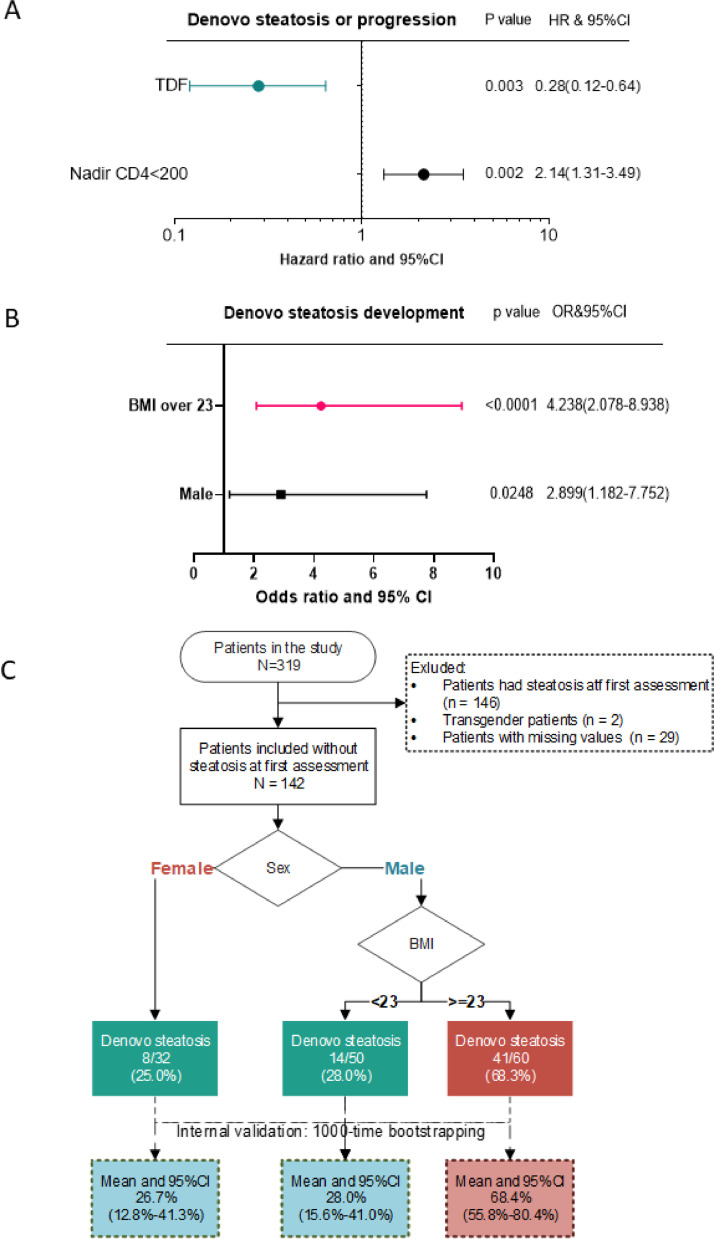
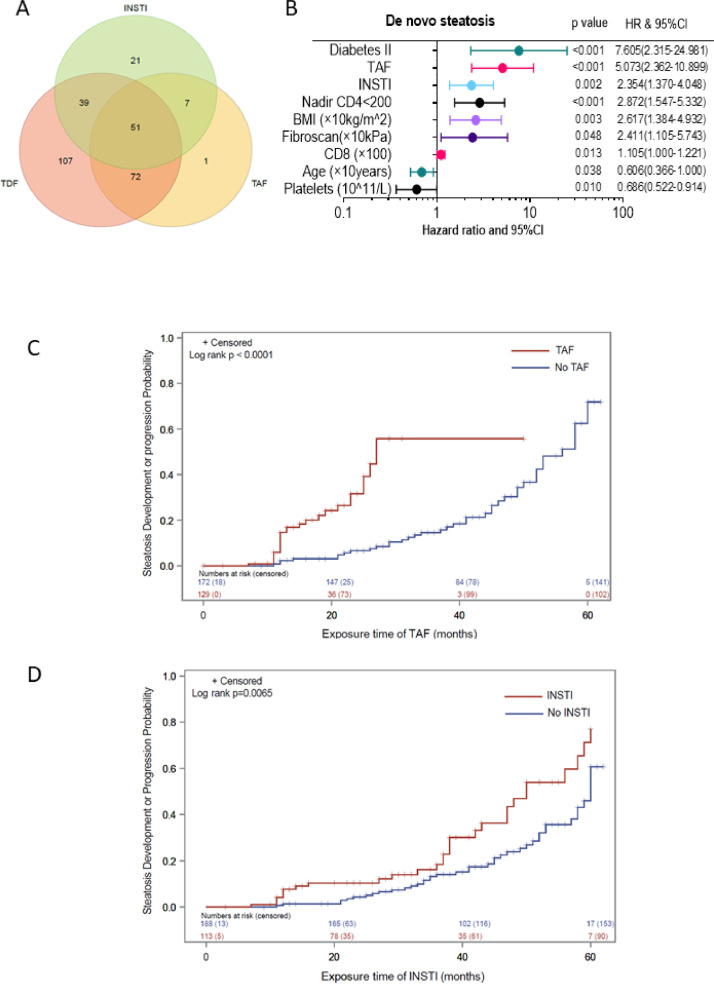
Findings: 319 monoinfected HIV positive patients with at least two visits were included into the study, of which 301 patients had at least two valid CAP measurements. 51·5%(155) patients did not have steatosis at first assessment, of which 45%(69) developed steatosis during follow-up. A BMI>23 kg/m2 (OR: 4·238, 95% CI: 2·078-8·938; p < 0·0001), tenofovir-alafenamid (TAF) (OR: 5·073, 95% CI: 2·362-10·899); p < 0·0001) and integrase strand transfer inhibitors (INSTI) (OR: 2·354, 95% CI: 1·370-4·048; p = 0·002), as well as type 2 diabetes mellitus (OR: 7·605, 95% CI: 2·315-24·981; p < 0·0001) were independent predictors of de novo steatosis in multivariable analysis. Tenofovir disoproxilfumarate (TDF) was associated with a lower risk for weight gain and steatosis progression/onset using CAP value (HR: 0·28, 95% CI: 0·12-0·64; p = 0·003) and FAST scores (HR: 0·31, 95% CI: 0·101-0·945; p = 0·04).
Interpretation: Steatosis can develop despite non-obese BMI in patients with HIV monoinfection under cART, especially in male patients with BMI over 23 kg/m2. While TAF and INSTI increase the risk of progression of steatosis, TDF was found to be independently associated with a lower risk of a clinically significant weight gain and thereby, might slow down development and progression of steatosis.
Funding: There was no additional funding received for this project. All funders mentioned in the 'declaration of interests' section had no influence on study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Keywords: APRI, AST to platelet ratio index; ART, antiretroviral treatment; AST, aspartate aminotransferase; BMI, body mass index; CAP, controlled attenuation parameter; Cap; DAA, direct-acting antiviral; FAST, FibroScan-AST; FIB4, fibrosis-4; HCV, chronic hepatitis C; Hiv; INSTI, integrase strand transfer inhibitors; NAFLD, Non-alcoholic fatty liver disease; NASH, non-alcoholic steatohepatitis; Nafld; PLHIV, people living with HIV; PrEP, pre-exposure prophylaxis; Steatosis; TAF, tenofovir-alafenamid; TDF, Tenofovir disoproxilfumarate; TE, transient elastography; cART.
© 2021 The Authors.
Conflict of interest statement
Jonel Trebicka is supported by grants from the Deutsche Forschungsgemeinschaft (SFB TRR57 to P18, CRC 1382AO9), European Union's Horizon 2020 Research and Innovation Programme (Galaxy, No. 668,031 and, MICROB-PREDICT, No. 825,694 and DECISION, No.847949), and Societal Challenges - Health, Demographic Change and Wellbeing (No. 731,875), and Cellex Foundation (PREDICT). Jürgen Rockstroh has received honoraria for consulting or speaking at educational events from Abivax, Galapagos, Gilead, Merck, Janssen, Theratechnologies and ViiV. Jenny Bischoff is supported by a scholarship of the BONFOR research support program for young scientists at the Rheinische Friedrich-Wilhelms-Universität (BONFOR Funding Instrument 1, Type A; Application number: 2020–1A-08). Christoph Boesecke has received honoraria for lectures from Abbvie, Gilead, ViiV, Janssen and MSD and was supported by a Grant from Hector-Stiftung for another HIV Study. Jan-Christian Wasmuth has received a travel grant from Gilead to attend a meeting. Wenyi Gu, Leona Dold, Carolynne Schwarze-Zander and Kathrin van Bremen have nothing to declare. All funders had no influence on study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Figures
References
-
- Guaraldi G., Squillace N., Stentarelli C. Nonalcoholic fatty liver disease in HIV-infected patients referred to a metabolic clinic: prevalence, characteristics, and predictors. Clin Infect Dis. 2008;47(2):250–257. - PubMed
-
- Vuille-Lessard E., Lebouche B., Lennox L. Nonalcoholic fatty liver disease diagnosed by transient elastography with controlled attenuation parameter in unselected HIV monoinfected patients. AIDS. 2016;30(17):2635–2643. - PubMed
-
- Iogna Prat L., Roccarina D., Lever R. Etiology and severity of liver disease in HIV-positive patients with suspected nafld: lessons from a cohort with available liver biopsies. J Acquir Immune Defic Syndr. 2019;80(4):474–480. - PubMed
-
- Maurice J.B., Patel A., Scott A.J., Patel K., Thursz M., Lemoine M. Prevalence and risk factors of nonalcoholic fatty liver disease in HIV-monoinfection. AIDS. 2017;31(11):1621–1632. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
