

Impact of the menstrual cycle on commercial prognostic gene signatures in oestrogen receptor-positive primary breast cancer
- PMID: 34524591
- PMCID: PMC8558287
- DOI: 10.1007/s10549-021-06377-3
Impact of the menstrual cycle on commercial prognostic gene signatures in oestrogen receptor-positive primary breast cancer
Abstract
Purpose: Changes occur in the expression of oestrogen-regulated and proliferation-associated genes in oestrogen receptor (ER)-positive breast tumours during the menstrual cycle. We investigated if Oncotype® DX recurrence score (RS), Prosigna® (ROR) and EndoPredict® (EP/EPclin) prognostic tests, which include some of these genes, vary according to the time in the menstrual cycle when they are measured.
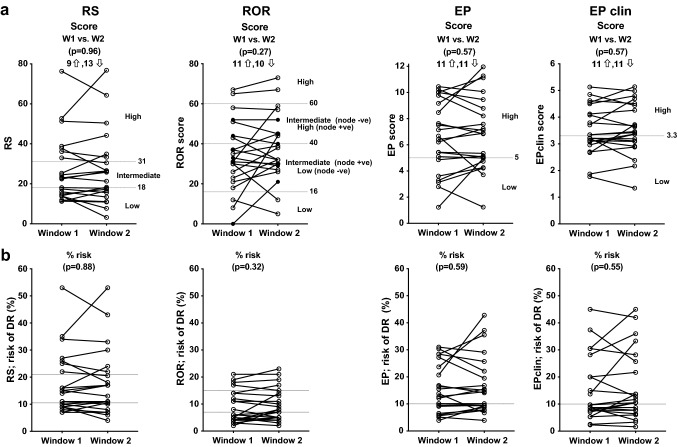
Methods: Pairs of test scores were derived from 30 ER-positive/human epidermal growth factor receptor-2-negative tumours sampled at two different points of the menstrual cycle. Menstrual cycle windows were prospectively defined as either W1 (days 1-6 and 27-35; low oestrogen and low progesterone) or W2 (days 7-26; high oestrogen and high or low progesterone).
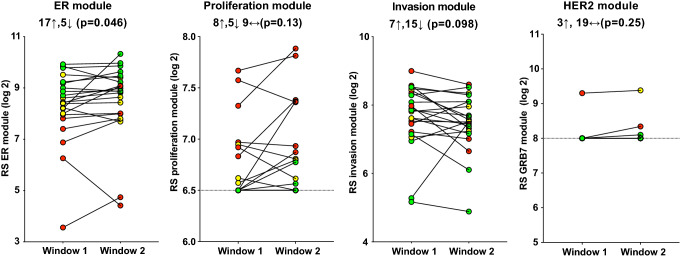
Results: The invasion module score of RS was lower (- 10.9%; p = 0.098), whereas the ER (+ 16.6%; p = 0.046) and proliferation (+ 7.3%; p = 0.13) module scores were higher in W2. PGR expression was significantly increased in W2 (+ 81.4%; p = 0.0029). Despite this, mean scores were not significantly different between W1 and W2 for any of the tests and the two measurements showed high correlation (r = 0.72-0.93). However, variability between the two measurements led to tumours being assigned to different risk categories in the following proportion of cases: RS 22.7%, ROR 27.3%, EP 13.6% and EPclin 13.6%.
Conclusion: There are significant changes during the menstrual cycle in the expression of some of the genes and gene module scores comprising the RS, ROR and EP/EPclin scores. These did not affect any of the prognostic scores in a systematic fashion, but there was substantial variability in paired measurements.
Keywords: Breast cancer; Hormone receptors; Menstrual cycle; Oestrogen-regulated genes; Prognostic signatures.
© 2021. The Author(s).
Conflict of interest statement
Mitch Dowsett received lecture fees from NanoString Technologies and served on an Agilent advisory board.
Figures


References
-
- Dodson A, Parry S, Ibrahim M, et al. Breast cancer biomarkers in clinical testing: analysis of a UK national external quality assessment scheme for immunocytochemistry and in situ hybridisation database containing results from 199 300 patients. J Pathol Clin Res. 2018;4:262–273. doi: 10.1002/cjp2.112. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
