

Nivolumab-induced membranous nephropathy in a patient with stage IV lung adenocarcinoma
- PMID: 34524642
- PMCID: PMC9061917
- DOI: 10.1007/s13730-021-00645-3
Nivolumab-induced membranous nephropathy in a patient with stage IV lung adenocarcinoma
Abstract
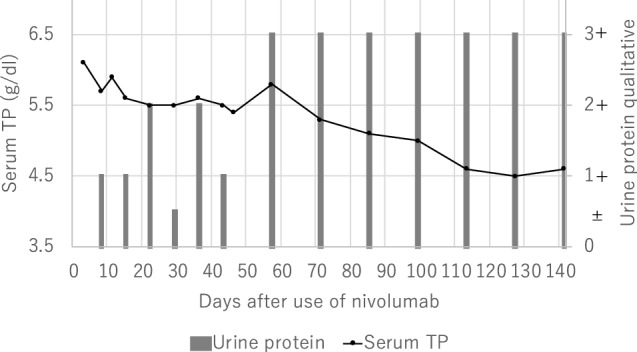
Immune check point inhibitors (ICIs) are now increasingly used for cancer therapy. At the same time, by activating the immune system, ICIs induce unique side effects, termed immune-related adverse events (irAEs). Renal irAEs, although uncommon, result in acute tubulointerstitial nephritis. Recently, because of an increase in ICI administration, renal irAEs, including glomerulonephritis, are being increasingly reported. A 69-year-old man presented with nephrotic syndrome after use of the ICI nivolumab. He underwent renal biopsy and was diagnosed with membranous nephropathy (MN) without acute tubulointerstitial nephritis. Immunofluorescence staining was negative for IgG4 and phospholipase A2 receptor (PLA2R), suggesting a malignancy-associated pattern. Oral glucocorticoid therapy was started as the standard treatment for irAEs, which resulted in complete remission of the nephrotic syndrome in 20 months. We suggest his MN was induced or accelerated by immune activation due to nivolumab. It means that ICIs possibly induce not only acute tubulointerstitial nephritis but also nephrotic syndrome due to MN as renal irAEs which is treatable with glucocorticoid.
Keywords: IgG subclass; Immune check point inhibitors (ICIs); Immune-related adverse events (irAEs); Membranous nephropathy (MN); Nephrotic syndrome; Nivolumab; Phospholipase A2 receptor (PLA2R).
© 2021. Japanese Society of Nephrology.
Conflict of interest statement
All the authors have declared that no Conflict of interest exists.
Figures






References
-
- Puzanov I, Diab A, Abdallah K, Bingham CO, 3rd, Brogdon C, Dadu R, et al. Managing toxicities associated with immune checkpoint inhibitors: consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. J Immunother Cancer. 2017;5(1):95. doi: 10.1186/s40425-017-0300-z. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
