

Juvenile myelomonocytic leukemia in the molecular era: a clinician's guide to diagnosis, risk stratification, and treatment
- PMID: 34525182
- PMCID: PMC8759142
- DOI: 10.1182/bloodadvances.2021005117
Juvenile myelomonocytic leukemia in the molecular era: a clinician's guide to diagnosis, risk stratification, and treatment
Abstract
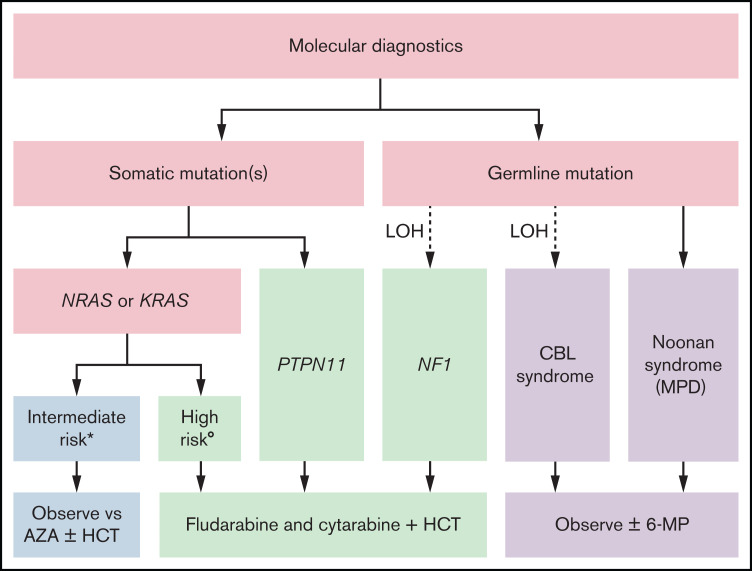
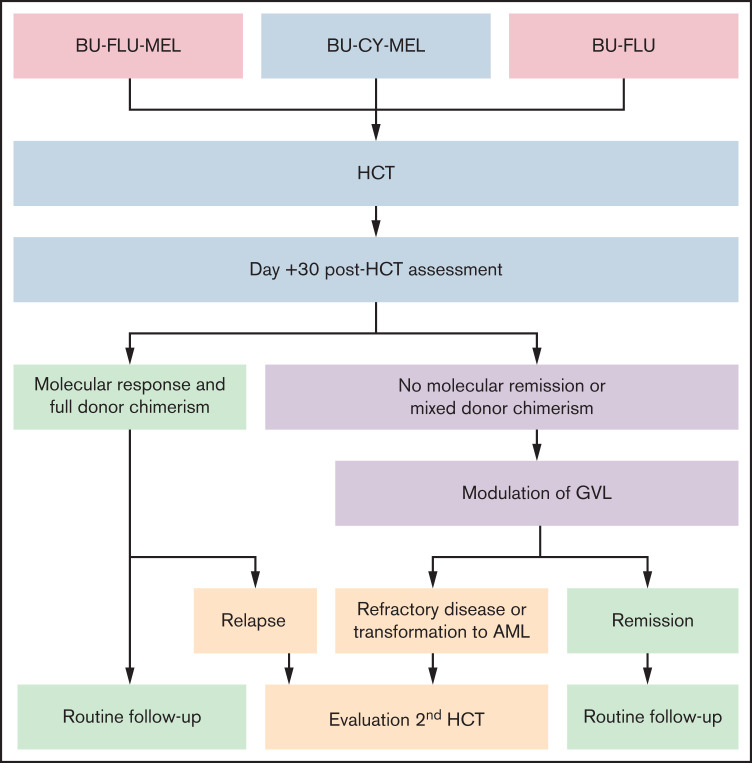
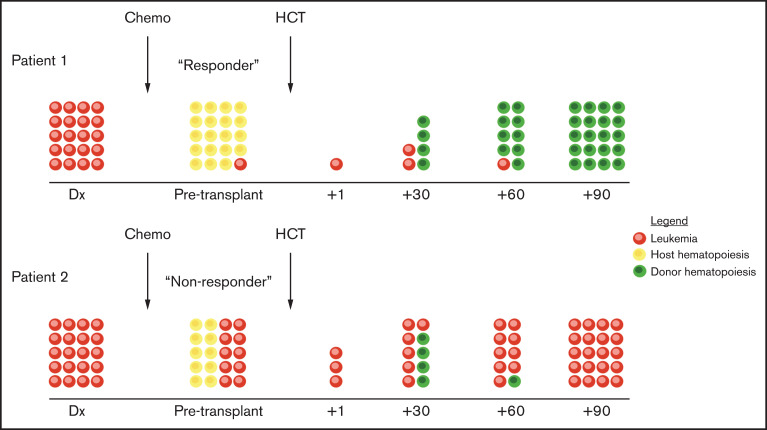
Juvenile myelomonocytic leukemia is an overlapping myeloproliferative and myelodysplastic disorder of early childhood . It is associated with a spectrum of diverse outcomes ranging from spontaneous resolution in rare patients to transformation to acute myeloid leukemia in others that is generally fatal. This unpredictable clinical course, along with initially descriptive diagnostic criteria, led to decades of productive international research. Next-generation sequencing now permits more accurate molecular diagnoses in nearly all patients. However, curative treatment is still reliant on allogeneic hematopoietic cell transplantation for most patients, and additional advances will be required to improve risk stratification algorithms that distinguish those that can be observed expectantly from others who require swift hematopoietic cell transplantation.
© 2021 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Figures
References
-
- Locatelli F, Niemeyer CM.. How I treat juvenile myelomonocytic leukemia. Blood. 2015;125(7):1083-1090. - PubMed
-
- Gupta RK, Qureshi A, Choi JK.. Histologic findings in skin biopsy in a JMML rash: a case report and review of literature. Pediatr Dev Pathol. 2014;17(2):130-133. - PubMed
-
- Niemeyer CM, Flotho C.. Juvenile myelomonocytic leukemia: who’s the driver at the wheel? Blood. 2019;133(10):1060-1070. - PubMed
-
- Arber DA, Orazi A, Hasserjian R, et al. . The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia [correction published in Blood. 2016;128(3):462–463]. Blood. 2016;127(20):2391-2405. - PubMed
-
- Hess JL, Zutter MM, Castleberry RP, Emanuel PD.. Juvenile chronic myelogenous leukemia. Am J Clin Pathol. 1996;105(2):238-248. - PubMed
