

The efficacy of corticosteroids therapy in patients with moderate to severe SARS-CoV-2 infection: a multicenter, randomized, open-label trial
- PMID: 34526033
- PMCID: PMC8441037
- DOI: 10.1186/s12931-021-01833-6
The efficacy of corticosteroids therapy in patients with moderate to severe SARS-CoV-2 infection: a multicenter, randomized, open-label trial
Abstract
Background: We performed a multicenter, randomized open-label trial in patients with moderate to severe Covid-19 treated with a range of possible treatment regimens.
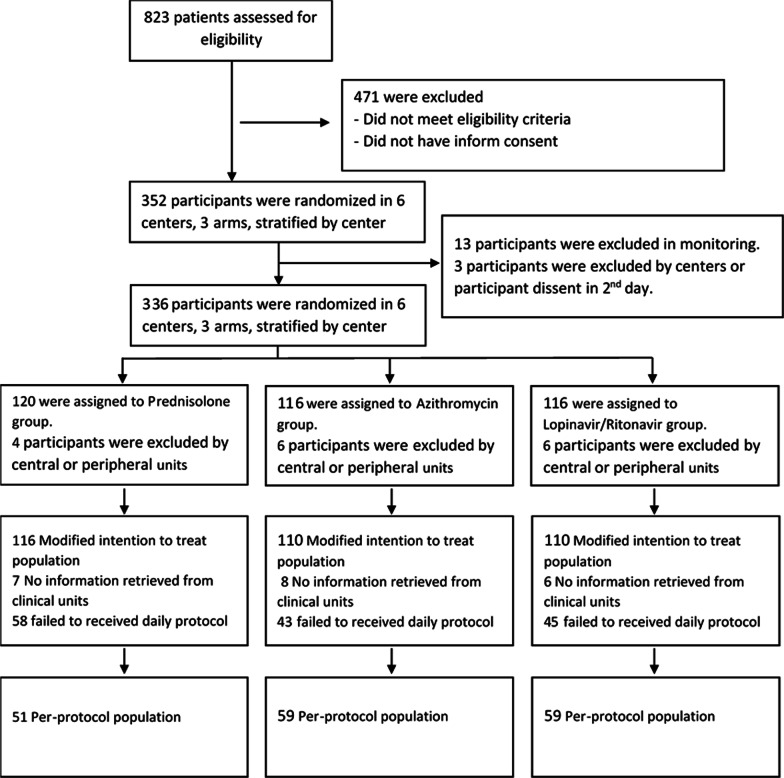
Methods: Patients were randomly assigned to one of three regimen groups at a ratio of 1:1:1. The primary outcome of this study was admission to the intensive care unit. Secondary outcomes were intubation, in-hospital mortality, time to clinical recovery, and length of hospital stay (LOS). Between April 13 and August 9, 2020, a total of 336 patients were randomly assigned to receive one of the 3 treatment regimens including group I (hydroxychloroquine stat, prednisolone, azithromycin and naproxen; 120 patients), group II (hydroxychloroquine stat, azithromycin and naproxen; 116 patients), and group III (hydroxychloroquine and lopinavir/ritonavir (116 patients). The mean LOS in patients receiving prednisolone was 5.5 in the modified intention-to-treat (mITT) population and 4.4 days in the per-protocol (PP) population compared with 6.4 days (mITT population) and 5.8 days (PP population) in patients treated with Lopinavir/Ritonavir.
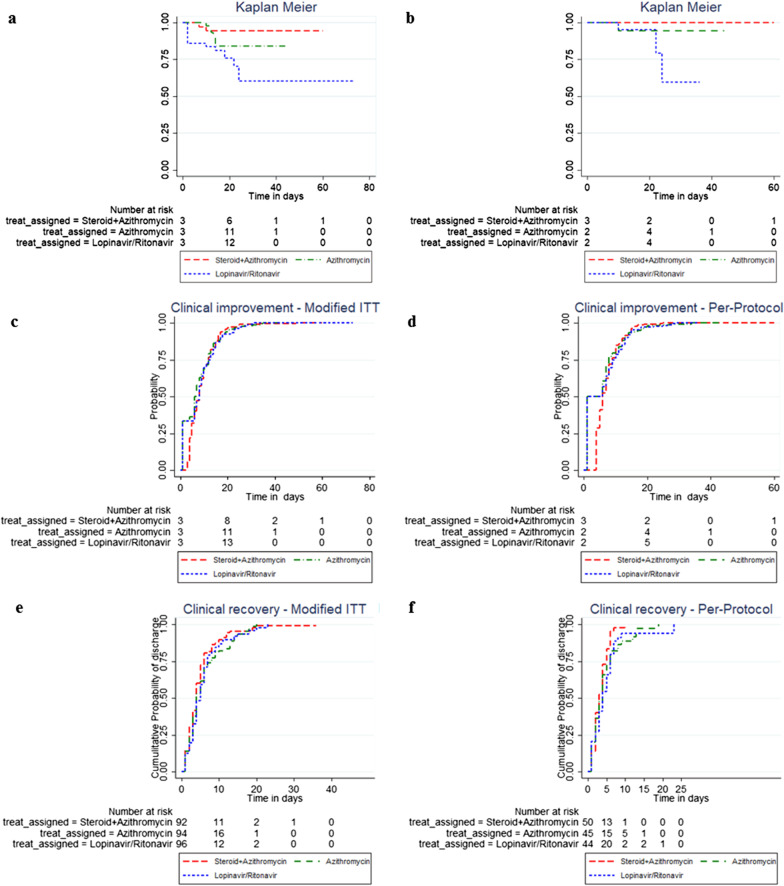
Results: The mean LOS was significantly lower in the mITT and PP populations who received prednisolone compared with populations treated with Lopinavir/Ritonavir (p = 0.028; p = 0.0007). We observed no significant differences in the number of deaths, ICU admission, and need for mechanical ventilation between the Modified ITT and per-protocol populations treated with prednisolone and Lopinavir/Ritonavir, although these outcomes were better in the arm treated with prednisolone. The time to clinical recovery was similar in the modified ITT and per-protocol populations treated with prednisolone, lopinavir/ritonavir, and azithromycin (P = 0.335; P = 0.055; p = 0.291; p = 0.098).
Conclusion: The results of the present study show that therapeutic regimen (regimen I) with low dose prednisolone was superior to other regimens in shortening the length of hospital stay in patients with moderate to severe COVID-19. The steroid sparing effect may be utilized to increase the effectiveness of corticosteroids in the management of diabetic patients by decreasing the dosage.
Keywords: Anti-inflammatory drugs; COVID-19; Corticosteroids; Low dose prednisolone.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Buja LM, Wolf DA, Zhao B, Akkanti B, McDonald M, Lelenwa L, et al. The emerging spectrum of cardiopulmonary pathology of the coronavirus disease 2019 (COVID-19): report of 3 autopsies from Houston, Texas, and review of autopsy findings from other United States cities. Cardiovasc Pathol. 2020;48:107233. doi: 10.1016/j.carpath.2020.107233. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
