

Stroke in Africa: profile, progress, prospects and priorities
- PMID: 34526674
- PMCID: PMC8441961
- DOI: 10.1038/s41582-021-00542-4
Stroke in Africa: profile, progress, prospects and priorities
Abstract
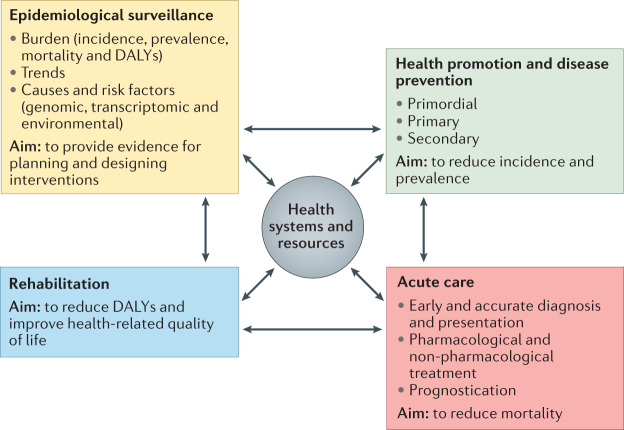
Stroke is a leading cause of disability, dementia and death worldwide. Approximately 70% of deaths from stroke and 87% of stroke-related disability occur in low-income and middle-income countries. At the turn of the century, the most common diseases in Africa were communicable diseases, whereas non-communicable diseases, including stroke, were considered rare, particularly in sub-Saharan Africa. However, evidence indicates that, today, Africa could have up to 2-3-fold greater rates of stroke incidence and higher stroke prevalence than western Europe and the USA. In Africa, data published within the past decade show that stroke has an annual incidence rate of up to 316 per 100,000, a prevalence of up to 1,460 per 100,000 and a 3-year fatality rate greater than 80%. Moreover, many Africans have a stroke within the fourth to sixth decades of life, with serious implications for the individual, their family and society. This age profile is particularly important as strokes in younger people tend to result in a greater loss of self-worth and socioeconomic productivity than in older individuals. Emerging insights from research into stroke epidemiology, genetics, prevention, care and outcomes offer great prospects for tackling the growing burden of stroke on the continent. In this article, we review the unique profile of stroke in Africa and summarize current knowledge on stroke epidemiology, genetics, prevention, acute care, rehabilitation, outcomes, cost of care and awareness. We also discuss knowledge gaps, emerging priorities and future directions of stroke medicine for the more than 1 billion people who live in Africa.
© 2021. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Mufunda J, et al. Emerging non-communicable disease epidemic in Africa: preventive measures from the WHO Regional Office for Africa. Ethn. Dis. 2006;16:521–526. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
