

Latest Evidence-Based Application for Radiofrequency Neurotomy (LEARN): Best Practice Guidelines from the American Society of Pain and Neuroscience (ASPN)
- PMID: 34526815
- PMCID: PMC8436449
- DOI: 10.2147/JPR.S325665
Latest Evidence-Based Application for Radiofrequency Neurotomy (LEARN): Best Practice Guidelines from the American Society of Pain and Neuroscience (ASPN)
Abstract
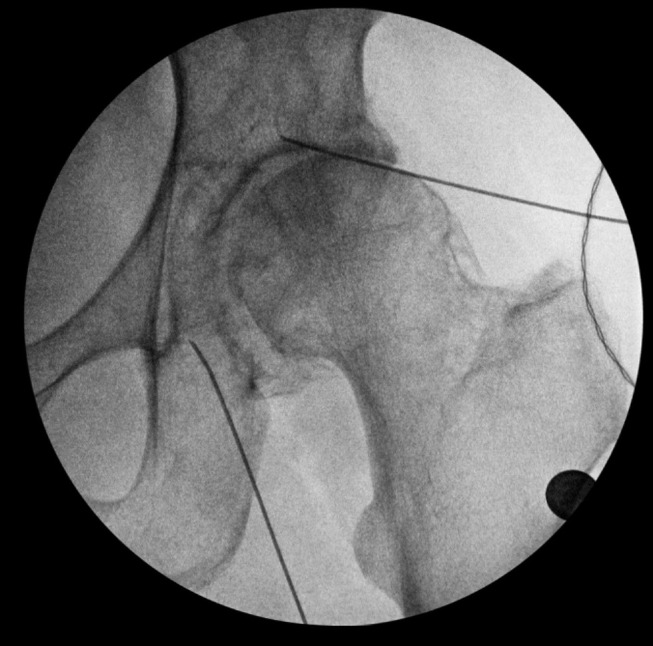
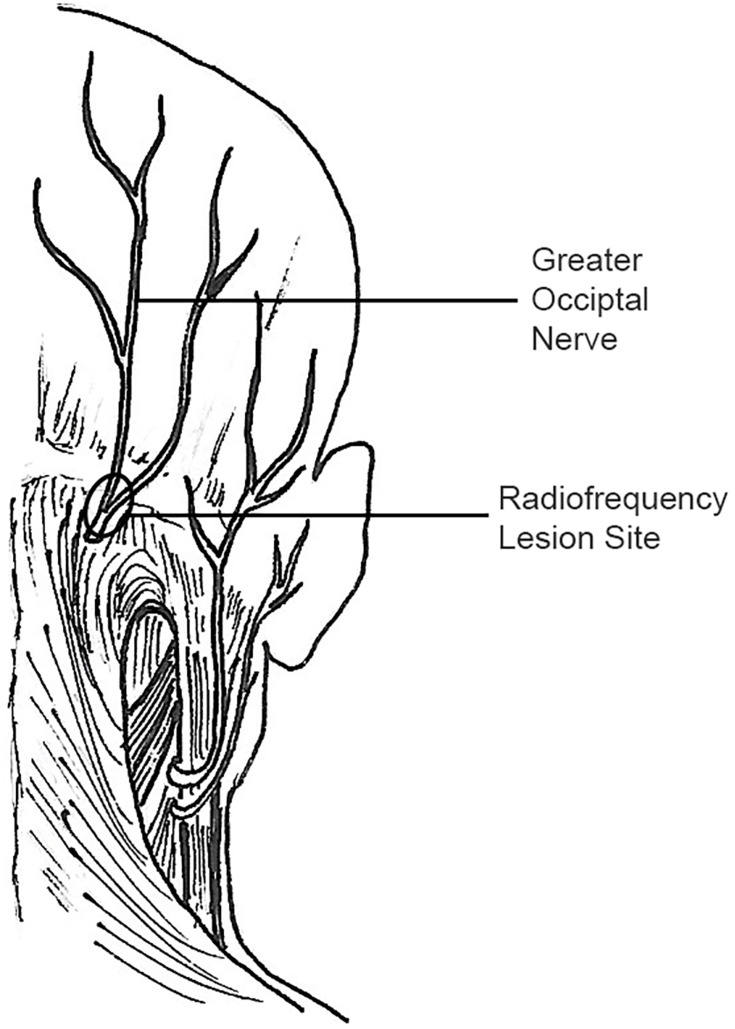
Radiofrequency neurotomy (RFN), also known as radiofrequency ablation (RFA), is a common interventional procedure used to treat pain from an innervated structure. RFN has historically been used to treat chronic facet-joint mediated pain. The use of RFN has more recently expanded beyond facet-joint mediated pain to peripherally innervated targets. In addition, there has also been the emergence of different radiofrequency modalities, including pulsed and cooled RFN. The use of RFN has been particularly important where conservative and/or surgical measures have failed to provide pain relief. With the emergence of this therapeutic option and its novel applications, the American Society of Pain and Neuroscience (ASPN) identified the need for formal evidence-based guidance. The authors formed a multidisciplinary work group tasked to examine the latest evidence-based medicine for the various applications of RFN, including cervical, thoracic, lumbar spine; posterior sacroiliac joint pain; hip and knee joints; and occipital neuralgia. Best practice guidelines, evidence and consensus grading were provided for each anatomical target.
Keywords: chronic pain; cooled ablation; occipital neuralgia; peripheral joint neurotomy; pulsed ablation; radiofrequency ablation; radiofrequency neurotomy; sacroiliac joint neurotomy.
© 2021 Lee et al.
Conflict of interest statement
Dr David W Lee reports grants from Abbott, during the conduct of the study; is a member of speakers Bureau for Abbott Neuromodulation, outside the submitted work. Dr Scott Pritzlaff reports personal fees from Nalu Medical, personal fees from EBT Medical, personal fees from SPR Therapeutics, outside the submitted work. Dr Jonathan M Hagedorn reports personal fees from Abbott, personal fees from Boston Scientific, personal fees from Nevro, personal fees from Speranza Therapeutics, outside the submitted work. Dr Jordan Tate reports personal fees from Abbott. Dr Dawood Sayed reports personal fees from Abbott, personal fees from Medtronic, personal fees from Nevro, PainTeq, Spr, and Vertos, during the conduct of the study. Dr Timothy R Deer reports personal fees from Abbott; also his institution research received funding from Avanos, outside the submitted work. The authors report no other conflicts of interest in this work.
Figures



References
-
- Krischner M. Zur elektrochirurgie[For electrosurgery]. Arch Klin Chir. 1931;147:761. German.
