

Foreign body aspiration
- PMID: 34527356
- PMCID: PMC8411180
- DOI: 10.21037/jtd.2020.03.94
Foreign body aspiration
Abstract
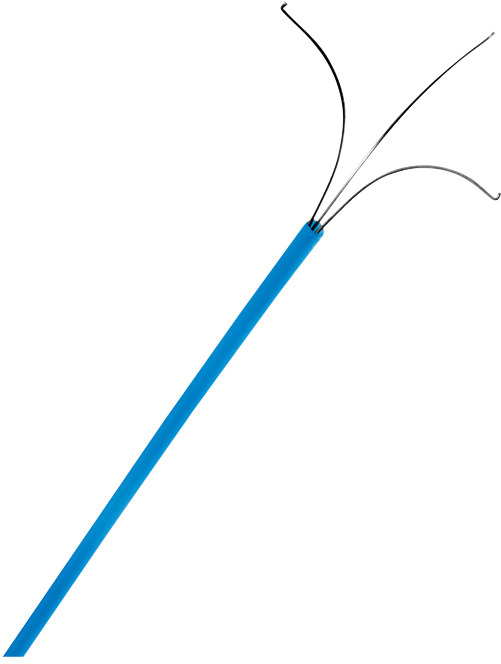
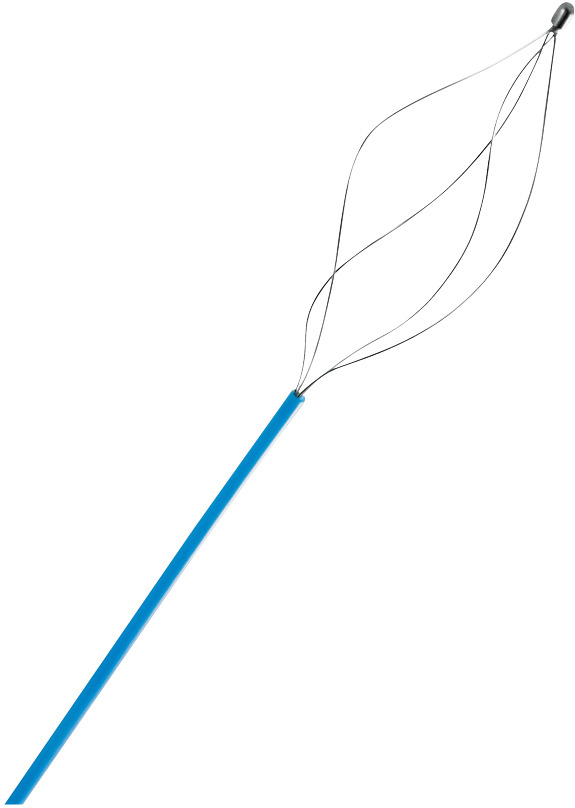
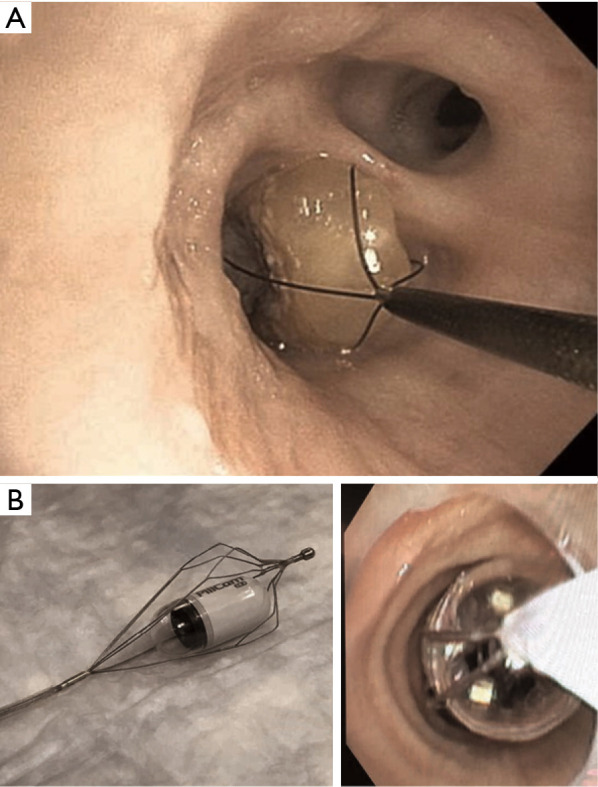
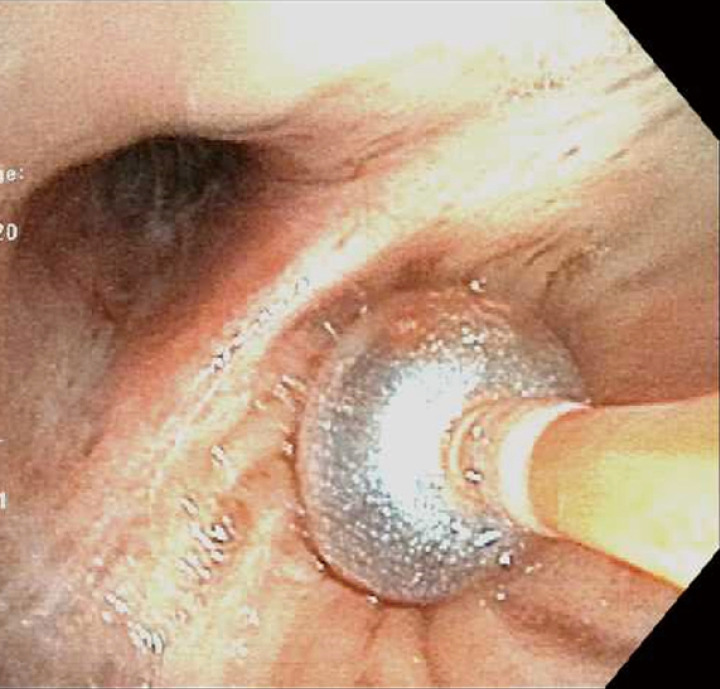
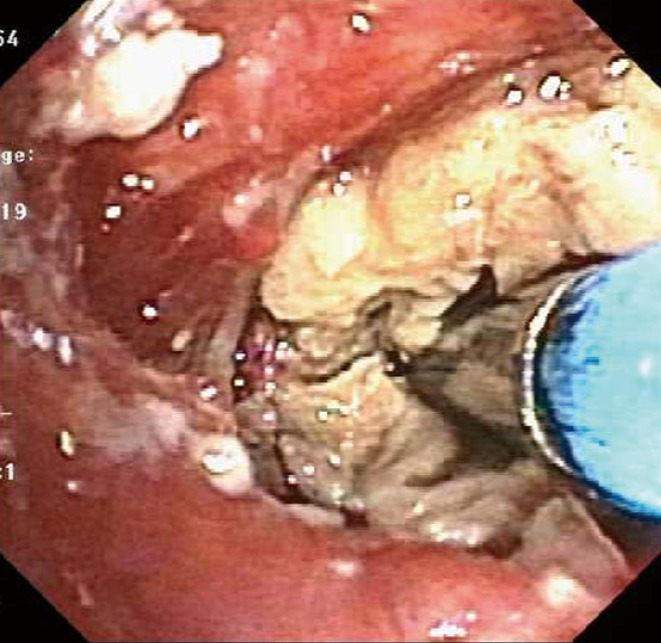
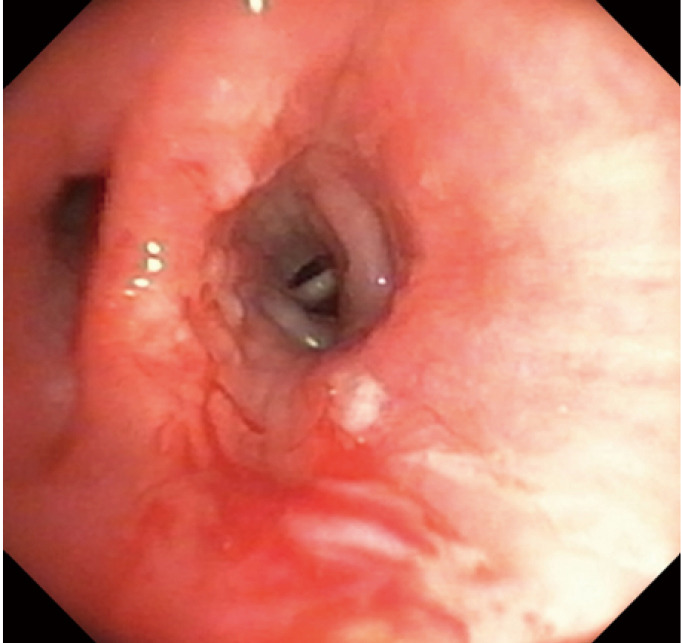
The clinical manifestations of foreign body (FB) aspiration can range from an asymptomatic presentation to a life-threatening emergency. Patients may present with acute onset cough, chest pain, breathlessness or sub-acutely with unexplained hemoptysis, non-resolving pneumonia and at times, as an incidental finding on imaging. Patients with iatrogenic FB such as an aspirated broken tooth during difficult intubation or a broken instrument are more common scenarios in the intensive care unit (ICU). Patients with post-obstructive pneumonia with or without sepsis, or variable degree of hemoptysis often require ICU level of care and bronchoscopic interventions. Rigid bronchoscopy has traditionally been the modality of choice; however, with the innovation in instrumentation and wider availability of flexible bronchoscopes, most of the FB removal is now successfully performed using flexible bronchoscopy. Proceduralists choose instruments in accordance with their training and expertise. We describe the use of most common instruments including forceps, balloon catheters, and baskets. Role of cryoprobe and LASER in FB removal is reviewed as well. In general, larger working channel bronchoscopes are preferred; however, smaller working channel bronchoscopes may be used in situations when the patients are intubated with a smaller diameter endotracheal or tracheostomy tubes. Large size FB are removed en bloc with the grasping tool, bronchoscope, and endotracheal or tracheostomy tube, requiring preparation to safely re-establish the airway. After FB removal, bronchoscopy is re-performed to identify any residual FB, assess any injury to the airway, suction post-obstructive secretions or pus, control any active bleeding and remove granulation tissue that may be obstructing the airway. Additional interventions like balloon dilatation may be required to dislodge an impacted FB or to maintain patency of bronchial lumen. If bronchoscopic methods fail, surgery may be required for retrieval of FB in symptomatic patients or to resect suppurative or necrotizing lung process. Multidisciplinary approach involving intensivists, surgeons, and anesthesiologists is the key to optimal patient outcomes.
Keywords: Foreign body (FB) aspiration; bronchoscopy; intensive care.
2021 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at: http://dx.doi.org/10.21037/jtd.2020.03.94). The series “Interventional Pulmonology in the Intensive Care Unit Environment” was commissioned by the editorial office without any funding or sponsorship. Ashutosh Sachdeva served as the unpaid Guest Editor of the series. The authors have no other conflicts of interest to declare.
Figures











References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials