

An overview of percutaneous endoscopic gastrostomy tube placement in the intensive care unit
- PMID: 34527366
- PMCID: PMC8411178
- DOI: 10.21037/jtd-19-3728
An overview of percutaneous endoscopic gastrostomy tube placement in the intensive care unit
Abstract
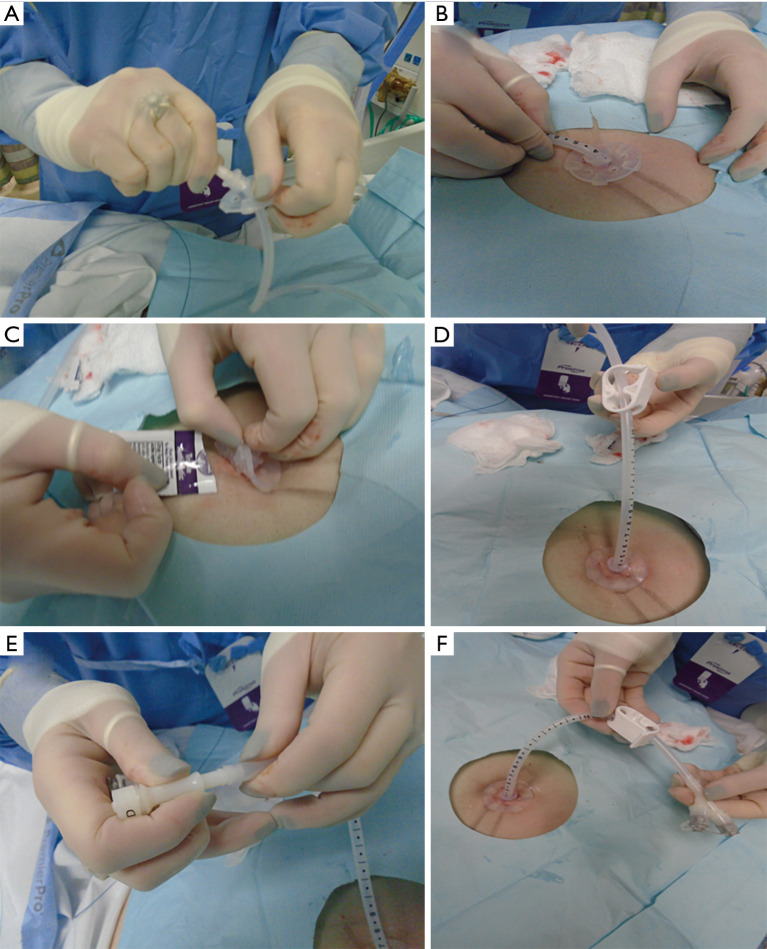
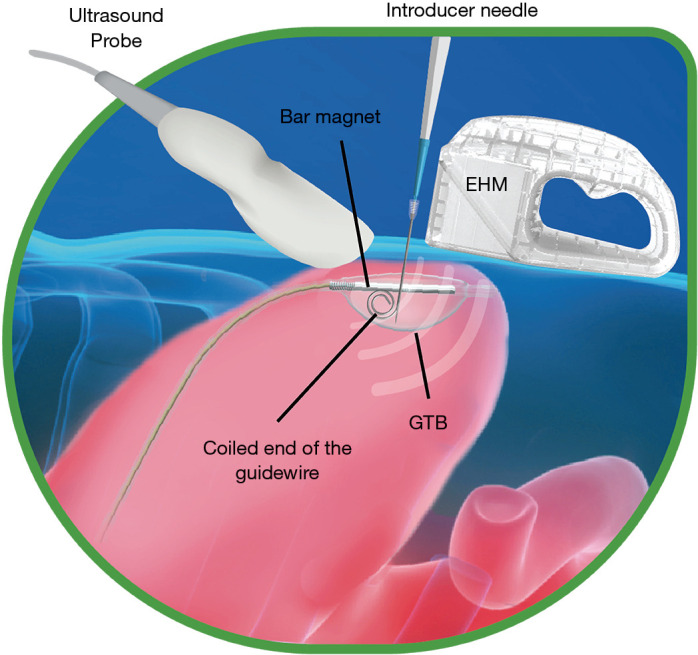
Critically ill patients are at increased risk for malnutrition as they often have underlying acute and chronic illness, stress related catabolism, decreased appetite, trauma and ongoing inflammation. Malnutrition is recognized as a leading cause of adverse outcomes, higher mortality, and increased hospital costs. Percutaneous endoscopic gastrostomy (PEG) tubes provide a safe and effective route to provide supplemental enteral nutrition to these patients. PEG placement has essentially replaced surgical gastrostomy as the modality of choice for longer term feeding in patients. This is a highly prevalent procedure with 160,000 to 200,000 PEG procedures performed each year in the United States. The purpose of this review is to provide an overview of current knowledge and practice standards with regards to placement of PEG tube in the Intensive Care Unit (ICU). When a patient is considered for a PEG tube, it is important to evaluate the treatment alternatives and identify the best option for each patient. In this review, we provide the advantages and disadvantages of various feeding modalities and devices. We review the indications and contraindications for PEG tube placement as well as the risks of this procedure. We then describe in detail the per-oral pull, per-oral push, and direct percutaneous techniques for PEG tube placement. Additionally, we review the feasibility of having interventional pulmonologists place PEG tubes in the ICU.
Keywords: Intensive Care Unit (ICU); Percutaneous endoscopic gastrostomy (PEG) placement; interventional pulmonology.
2021 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form, available at: http://dx.doi.org/10.21037/jtd-19-3728. The series “Interventional Pulmonology in the Intensive Care Unit Environment” was commissioned by the editorial office without any funding sponsorship. The authors have no other conflicts of interest to declare.
Figures




References
-
- Gauderer MW, Ponsky JL, Izant RJ, Jr. Gastrostomy without laparotomy: a percutaneous endoscopic technique 1980. Nutrition 1998;14:736-8. - PubMed