

Hypophysitis, the Growing Spectrum of a Rare Pituitary Disease
- PMID: 34528683
- PMCID: PMC8684465
- DOI: 10.1210/clinem/dgab672
Hypophysitis, the Growing Spectrum of a Rare Pituitary Disease
Abstract
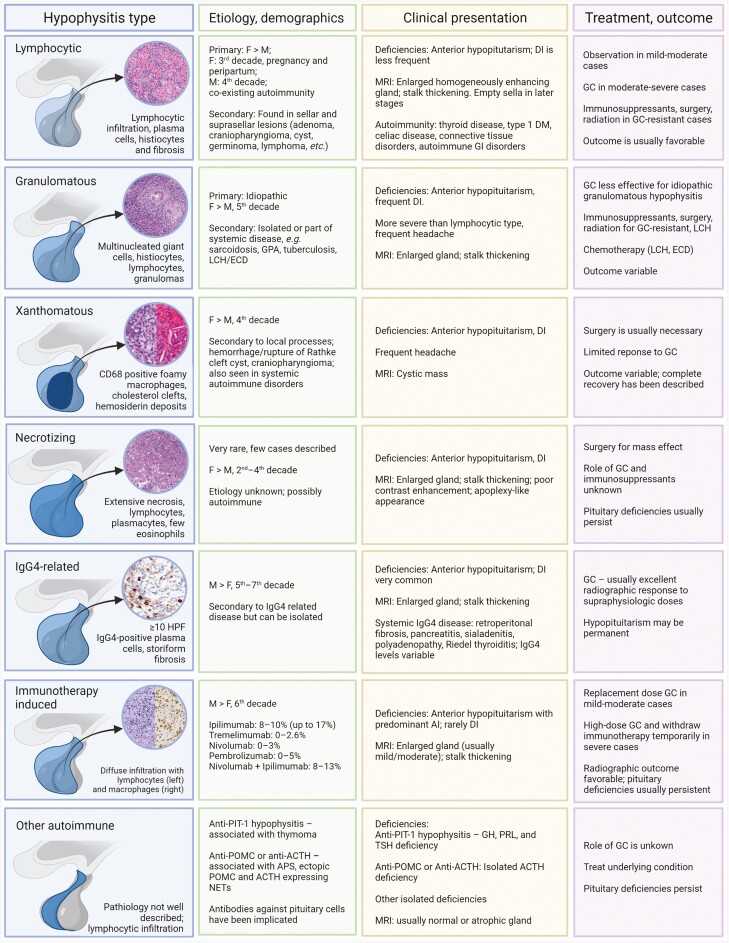
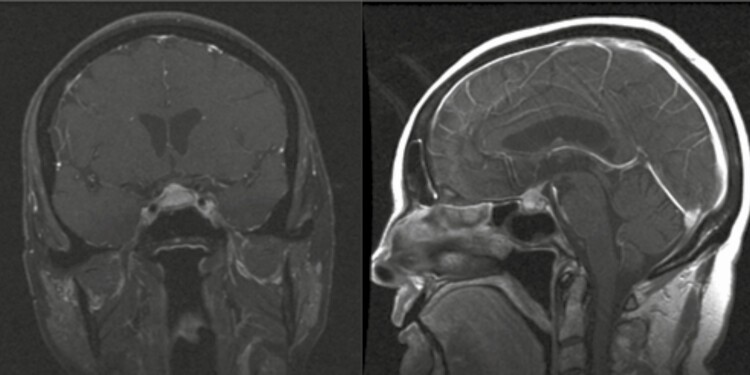
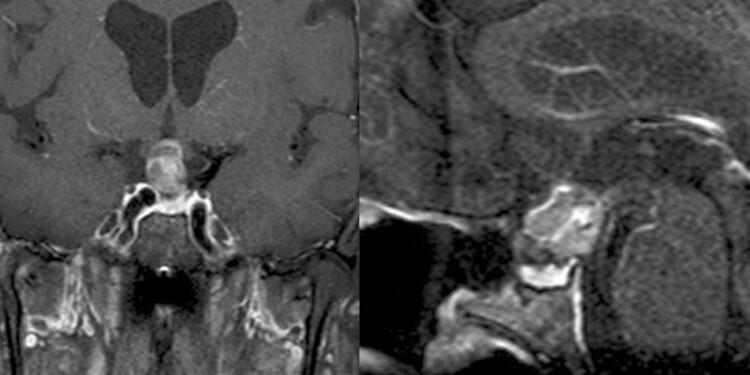
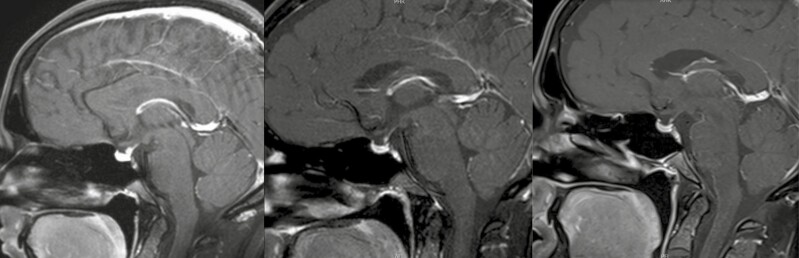
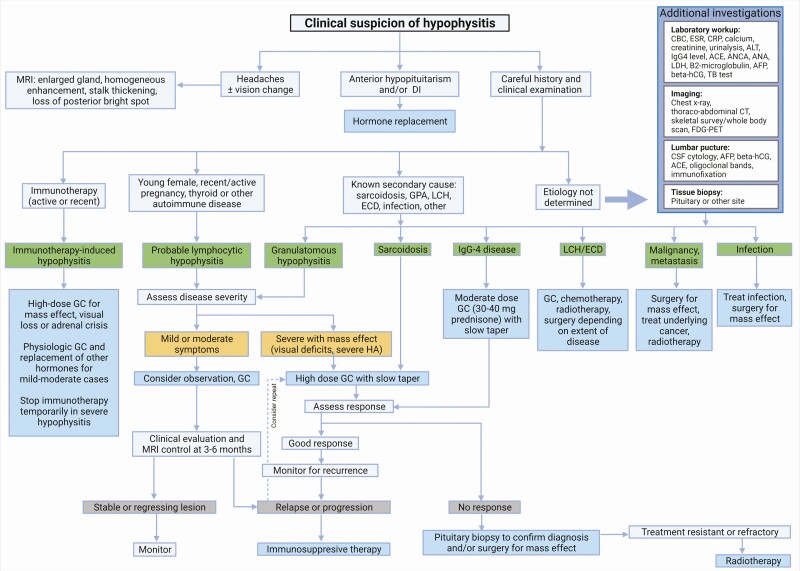
Hypophysitis is defined as inflammation of the pituitary gland that is primary or secondary to a local or systemic process. Differential diagnosis is broad (including primary tumors, metastases, and lympho-proliferative diseases) and multifaceted. Patients with hypophysitis typically present with headaches, some degree of anterior and/or posterior pituitary dysfunction, and enlargement of pituitary gland and/or stalk, as determined by imaging. Most hypophysitis causes are autoimmune, but other etiologies include inflammation secondary to sellar tumors or cysts, systemic diseases, and infection or drug-induced causes. Novel pathologies such as immunoglobulin G4-related hypophysitis, immunotherapy-induced hypophysitis, and paraneoplastic pituitary-directed autoimmunity are also included in a growing spectrum of this rare pituitary disease. Typical magnetic resonance imaging reveals stalk thickening and homogenous enlargement of the pituitary gland; however, imaging is not always specific. Diagnosis can be challenging, and ultimately, only a pituitary biopsy can confirm hypophysitis type and rule out other etiologies. A presumptive diagnosis can be made often without biopsy. Detailed history and clinical examination are essential, notably for signs of underlying etiology with systemic manifestations. Hormone replacement and, in selected cases, careful observation is advised with imaging follow-up. High-dose glucocorticoids are initiated mainly to help reduce mass effect. A response may be observed in all auto-immune etiologies, as well as in lymphoproliferative diseases, and, as such, should not be used for differential diagnosis. Surgery may be necessary in some cases to relieve mass effect and allow a definite diagnosis. Immunosuppressive therapy and radiation are sometimes also necessary in resistant cases.
Keywords: IgG4-related hypophysitis; hypophysitis; immunotherapy-induced hypophysitis; lymphocytic hypophysitis; paraneoplastic pituitary-directed autoimmunity; stalk biopsy.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
Comment in
-
Letter to the Editor From Asa and Mete: "Hypophysitis, the Growing Spectrum of a Rare Pituitary Disease".J Clin Endocrinol Metab. 2022 May 17;107(6):e2649. doi: 10.1210/clinem/dgac025. J Clin Endocrinol Metab. 2022. PMID: 35037041 No abstract available.
-
Response to Letter to the Editor From Asa and Mete: "Hypophysitis, the Growing Spectrum of a Rare Pituitary Disease".J Clin Endocrinol Metab. 2022 Apr 19;107(5):e2208-e2209. doi: 10.1210/clinem/dgac026. J Clin Endocrinol Metab. 2022. PMID: 35037055 Free PMC article. No abstract available.
-
Letter to the Editor From Kelestimur et al.: "Hypophysitis, the Growing Spectrum of a Rare Pituitary Disease".J Clin Endocrinol Metab. 2022 May 17;107(6):e2640-e2641. doi: 10.1210/clinem/dgac134. J Clin Endocrinol Metab. 2022. PMID: 35259231 No abstract available.
References
-
- Caturegli P, Newschaffer C, Olivi A, Pomper MG, Burger PC, Rose NR. Autoimmune hypophysitis. Endocr Rev. 2005;26(5):599-614. - PubMed
-
- Bando H, Iguchi G, Fukuoka H, et al. The prevalence of IgG4-related hypophysitis in 170 consecutive patients with hypopituitarism and/or central diabetes insipidus and review of the literature. Eur J Endocrinol. 2014;170(2):161-172. - PubMed
-
- Faje A. Immunotherapy and hypophysitis: clinical presentation, treatment, and biologic insights. Pituitary. 2016;19(1):82-92. - PubMed
-
- Türe U, De Bellis A, Harput MV, et al. Hypothalamitis: a novel autoimmune endocrine disease. a literature review and case report. J Clin Endocrinol Metab 2020;106(2): e415-e429. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
