

Association of coronary artery calcium score with qualitatively and quantitatively assessed adverse plaque on coronary CT angiography in the SCOT-HEART trial
- PMID: 34529050
- PMCID: PMC9612790
- DOI: 10.1093/ehjci/jeab135
Association of coronary artery calcium score with qualitatively and quantitatively assessed adverse plaque on coronary CT angiography in the SCOT-HEART trial
Abstract
Aims: Coronary artery calcification is a marker of cardiovascular risk, but its association with qualitatively and quantitatively assessed plaque subtypes is unknown.
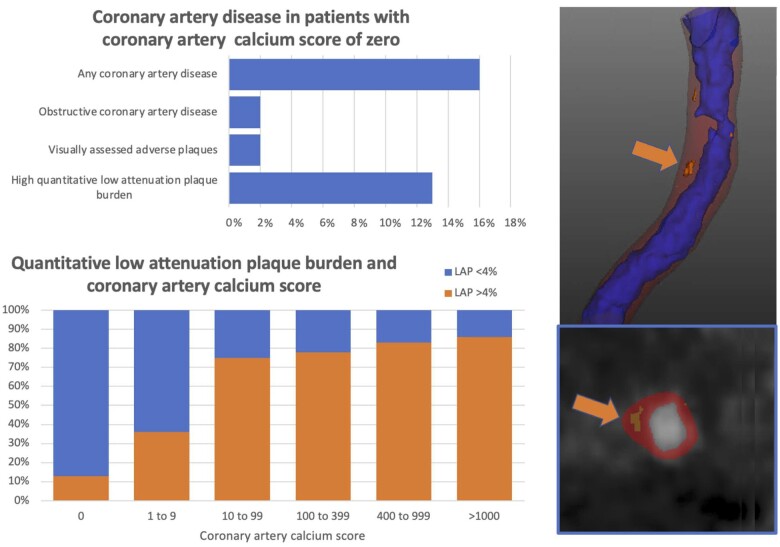
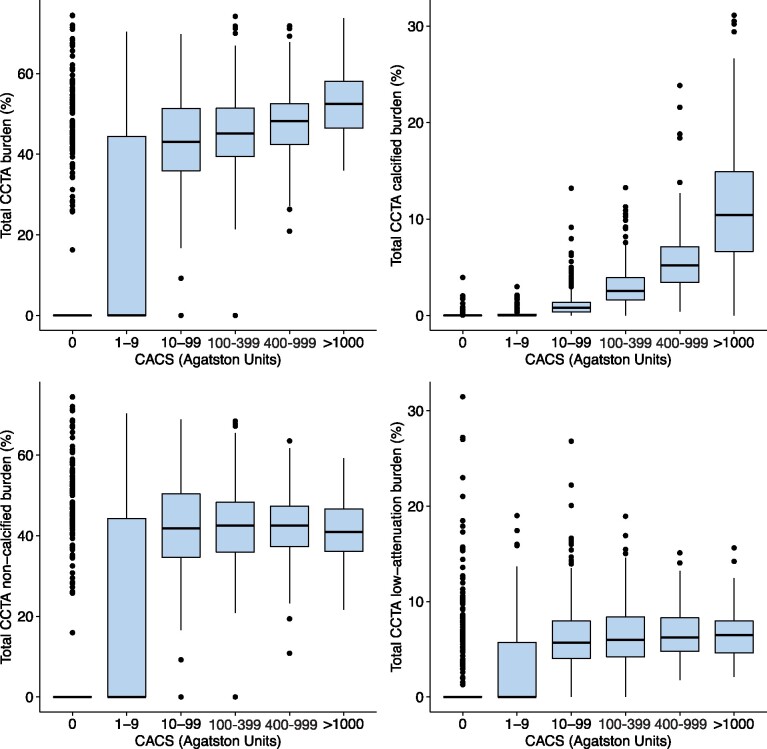
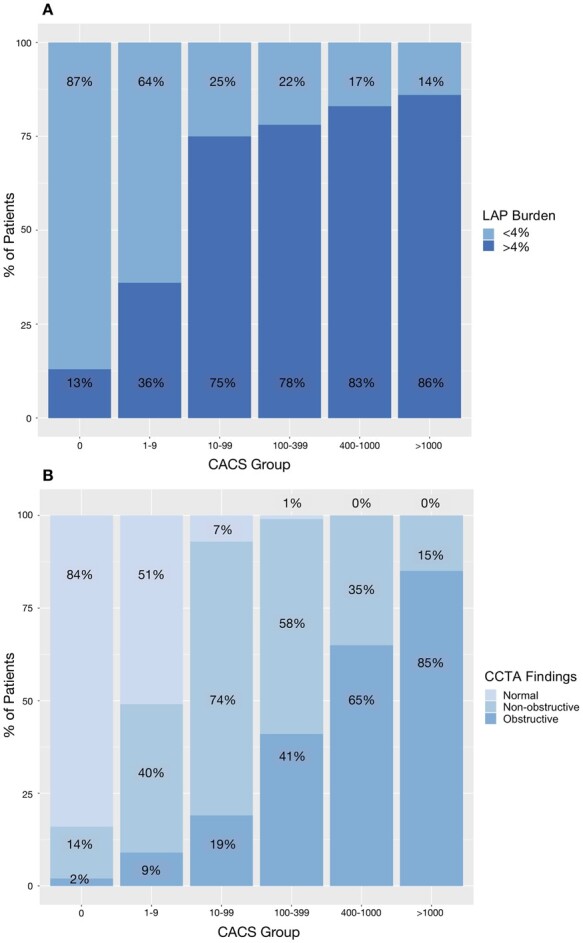
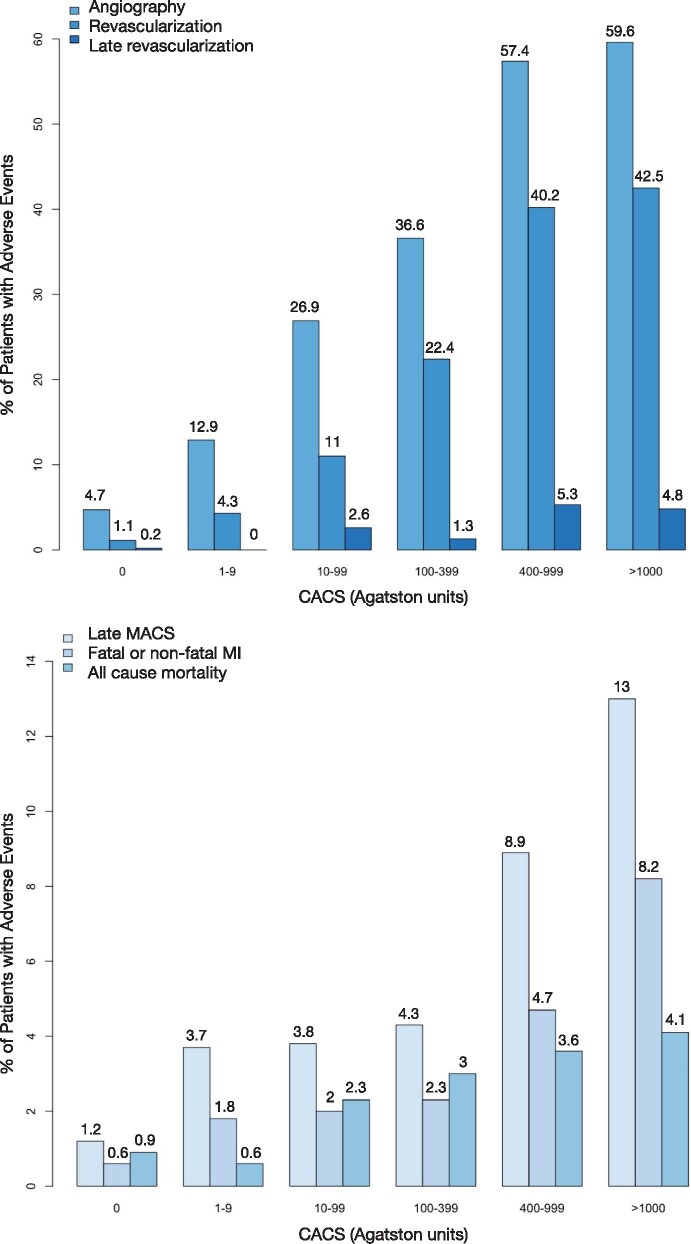
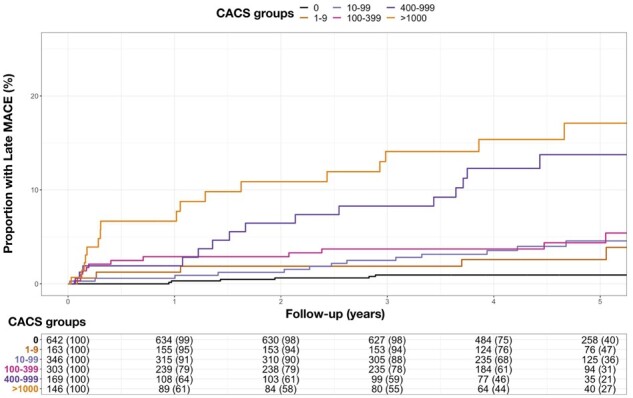
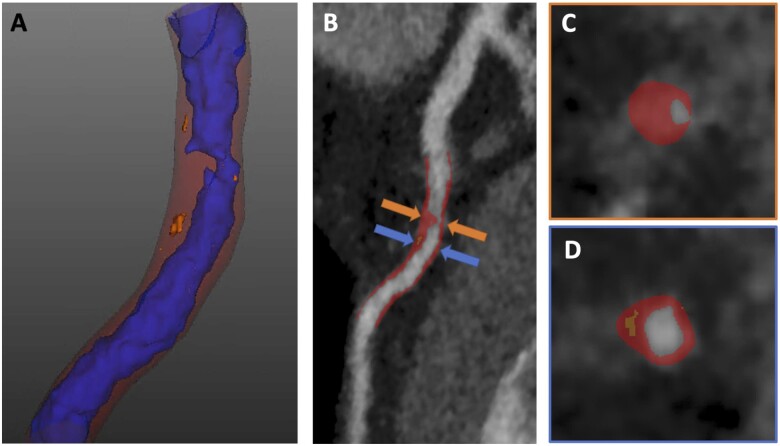
Methods and results: In this post-hoc analysis, computed tomography (CT) images and 5-year clinical outcomes were assessed in SCOT-HEART trial participants. Agatston coronary artery calcium score (CACS) was measured on non-contrast CT and was stratified as zero (0 Agatston units, AU), minimal (1-9 AU), low (10-99 AU), moderate (100-399 AU), high (400-999 AU), and very high (≥1000 AU). Adverse plaques were investigated by qualitative (visual categorization of positive remodelling, low-attenuation plaque, spotty calcification, and napkin ring sign) and quantitative (calcified, non-calcified, low-attenuation, and total plaque burden; Autoplaque) assessments. Of 1769 patients, 36% had a zero, 9% minimal, 20% low, 17% moderate, 10% high, and 8% very high CACS. Amongst patients with a zero CACS, 14% had non-obstructive disease, 2% had obstructive disease, 2% had visually assessed adverse plaques, and 13% had low-attenuation plaque burden >4%. Non-calcified and low-attenuation plaque burden increased between patients with zero, minimal, and low CACS (P < 0.001), but there was no statistically significant difference between those with medium, high, and very high CACS. Myocardial infarction occurred in 41 patients, 10% of whom had zero CACS. CACS >1000 AU and low-attenuation plaque burden were the only predictors of myocardial infarction, independent of obstructive disease, and 10-year cardiovascular risk score.
Conclusion: In patients with stable chest pain, zero CACS is associated with a good but not perfect prognosis, and CACS cannot rule out obstructive coronary artery disease, non-obstructive plaque, or adverse plaque phenotypes, including low-attenuation plaque.
Keywords: atherosclerotic plaque; computed tomography; computed tomography coronary angiography; coronary calcium score; low-attenuation plaque.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2021. For permissions, please email: journals.permissions@oup.com.
Conflict of interest statement
Conflict of interest: D.D., P.S., S.C., and D.S.B. may receive software royalties from Cedars-Sinai Medical Center, and D.D., P.S., and D.S.B. have a patent. Outside the submitted work, E.v.B. reports personal fees from Aidence NV, Mentholatum, grants from Siemens Healthineers, and other from QCTIS, Astra Zeneca, and Roche Diagnostics. D.E.N. reports grants from Chief Scientist Office, British Heart Foundation, and Royal Bank of Scotland and personal fees from Toshiba during the conduct of the study. Outside the submitted work, P.J.S. reports grants from NIH, Siemens Medical Systems, and Amazon Web Services. The remaining authors have nothing to disclose.
Figures
References
-
- Sarwar A, Shaw LJ, Shapiro MD, Blankstein R, Hoffmann U, Cury RCet al. . Diagnostic and prognostic value of absence of coronary artery calcification. JACC Cardiovasc Imaging 2009;2:675–88. - PubMed
-
- Hecht HS, Blaha MJ, Kazerooni EA, Cury RC, Budoff M, Leipsic Jet al. . CAC-DRS: coronary artery calcium data and reporting system. An expert consensus document of the Society of Cardiovascular Computed Tomography (SCCT). J Cardiovasc Comput Tomogr 2018;12:185–91. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- CH/F/21/90010/BHF_/British Heart Foundation/United Kingdom
- FS/16/14/32023/BHF_/British Heart Foundation/United Kingdom
- G0701127/MRC_/Medical Research Council/United Kingdom
- FS/17/79/33226/BHF_/British Heart Foundation/United Kingdom
- RG/20/10/34966/BHF_/British Heart Foundation/United Kingdom
- RE/18/5/34216/BHF_/British Heart Foundation/United Kingdom
- AA/18/3/34220/BHF_/British Heart Foundation/United Kingdom
- R01 HL151266/HL/NHLBI NIH HHS/United States
- CH/09/002/26360/BHF_/British Heart Foundation/United Kingdom
- CS/18/4/34074/BHF_/British Heart Foundation/United Kingdom
- FS/14/78/31020/BHF_/British Heart Foundation/United Kingdom
- RG/16/10/32375/BHF_/British Heart Foundation/United Kingdom
- CH/09/002/BHF_/British Heart Foundation/United Kingdom
- PCL/17/04/CSO_/Chief Scientist Office/United Kingdom
- FS/ICRF/20/26002/BHF_/British Heart Foundation/United Kingdom
- CZH/4/1135/CSO_/Chief Scientist Office/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
