

Role of total lung stress on the progression of early COVID-19 pneumonia
- PMID: 34529118
- PMCID: PMC8444534
- DOI: 10.1007/s00134-021-06519-7
Role of total lung stress on the progression of early COVID-19 pneumonia
Erratum in
-
Correction to: Role of total lung stress on the progression of early COVID‑19 pneumonia.Intensive Care Med. 2022 Mar;48(3):387-388. doi: 10.1007/s00134-021-06589-7. Intensive Care Med. 2022. PMID: 34905078 Free PMC article. No abstract available.
Abstract
Purpose: We investigated if the stress applied to the lung during non-invasive respiratory support may contribute to the coronavirus disease 2019 (COVID-19) progression.
Methods: Single-center, prospective, cohort study of 140 consecutive COVID-19 pneumonia patients treated in high-dependency unit with continuous positive airway pressure (n = 131) or non-invasive ventilation (n = 9). We measured quantitative lung computed tomography, esophageal pressure swings and total lung stress.
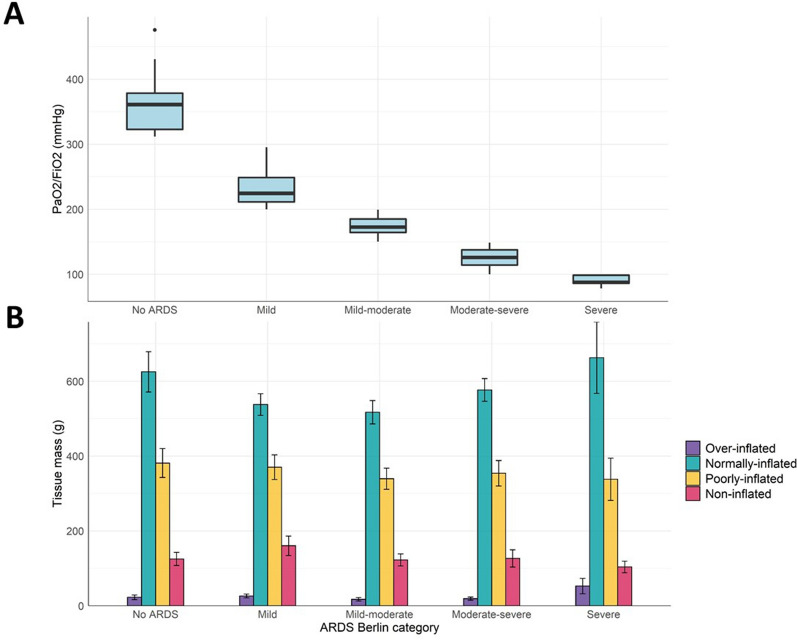
Results: Patients were divided in five subgroups based on their baseline PaO2/FiO2 (day 1): non-CARDS (median PaO2/FiO2 361 mmHg, IQR [323-379]), mild (224 mmHg [211-249]), mild-moderate (173 mmHg [164-185]), moderate-severe (126 mmHg [114-138]) and severe (88 mmHg [86-99], p < 0.001). Each subgroup had similar median lung weight: 1215 g [1083-1294], 1153 [888-1321], 968 [858-1253], 1060 [869-1269], and 1127 [937-1193] (p = 0.37). They also had similar non-aerated tissue fraction: 10.4% [5.9-13.7], 9.6 [7.1-15.8], 9.4 [5.8-16.7], 8.4 [6.7-12.3] and 9.4 [5.9-13.8], respectively (p = 0.85). Treatment failure of CPAP/NIV occurred in 34 patients (24.3%). Only three variables, at day one, distinguished patients with negative outcome: PaO2/FiO2 ratio (OR 0.99 [0.98-0.99], p = 0.02), esophageal pressure swing (OR 1.13 [1.01-1.27], p = 0.032) and total stress (OR 1.17 [1.06-1.31], p = 0.004). When these three variables were evaluated together in a multivariate logistic regression analysis, only the total stress was independently associated with negative outcome (OR 1.16 [1.01-1.33], p = 0.032).
Conclusions: In early COVID-19 pneumonia, hypoxemia is not linked to computed tomography (CT) pathoanatomy, differently from typical ARDS. High lung stress was independently associated with the failure of non-invasive respiratory support.
Keywords: ARDS; COVID-19; Computed tomography scan; Lung stress; Mechanical ventilation; Non-invasive respiratory support; Ventilation-induced lung injury.
© 2021. The Author(s).
Conflict of interest statement
LG reports a consultancy for General Electrics and SIDAM. He also receives lecture fees from Estor and Dimar. LS reports financial relationships with Medtronic, Ferrer Deutschland and Merck.
Figures

Comment in
-
Role of total lung stress on the progression of early COVID-19 pneumonia: collinearity and potential confounders.Intensive Care Med. 2022 Feb;48(2):249-250. doi: 10.1007/s00134-021-06557-1. Epub 2021 Oct 27. Intensive Care Med. 2022. PMID: 34705080 Free PMC article. No abstract available.
References
-
- Chiumello D, Busana M, Coppola S, Romitti F, Formenti P, Bonifazi M, Pozzi T, Palumbo MM, Cressoni M, Herrmann P, Meissner K, Quintel M, Camporota L, Marini JJ, Gattinoni L. Physiological and quantitative CT-scan characterization of COVID-19 and typical ARDS: a matched cohort study. Intensive Care Med. 2020 doi: 10.1007/s00134-020-06281-2. - DOI - PMC - PubMed
