

Identification of immune correlates of fatal outcomes in critically ill COVID-19 patients
- PMID: 34529726
- PMCID: PMC8445447
- DOI: 10.1371/journal.ppat.1009804
Identification of immune correlates of fatal outcomes in critically ill COVID-19 patients
Abstract
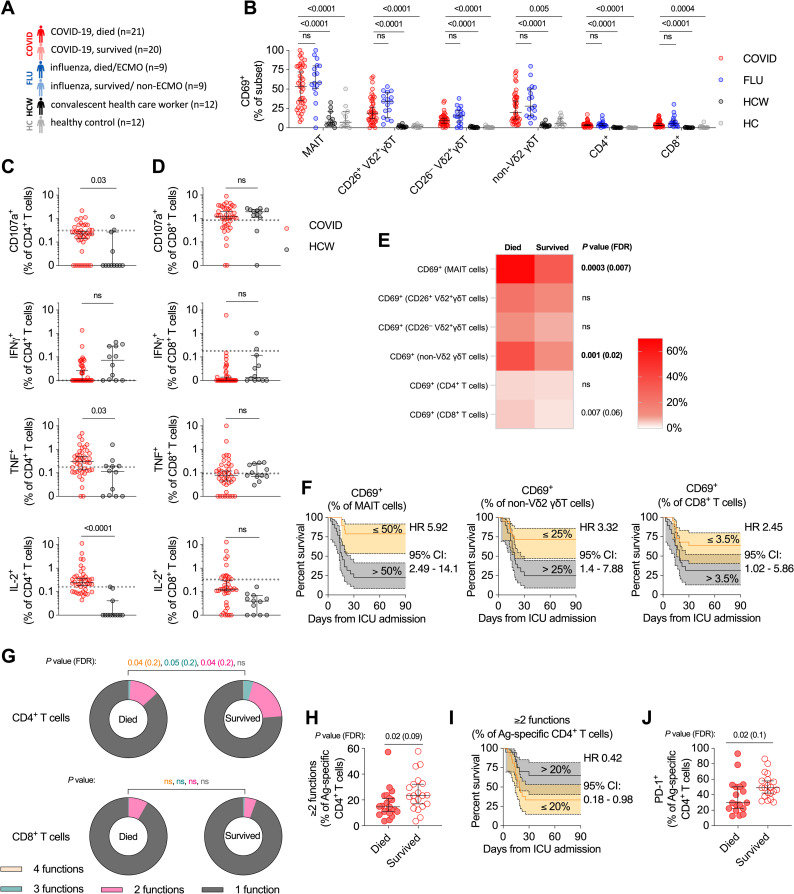
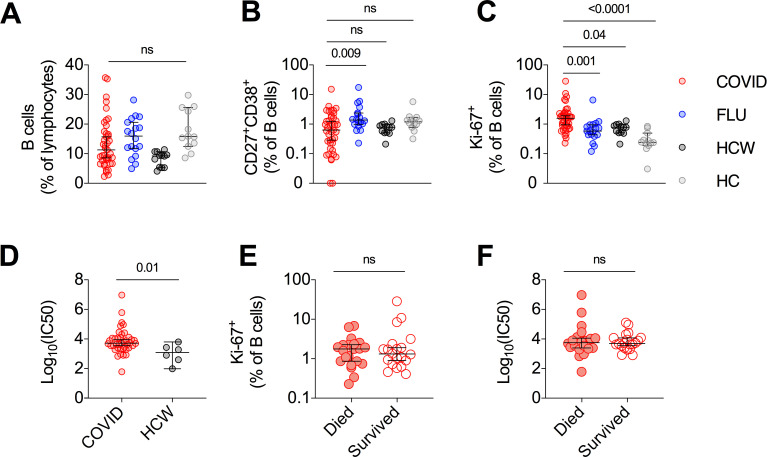
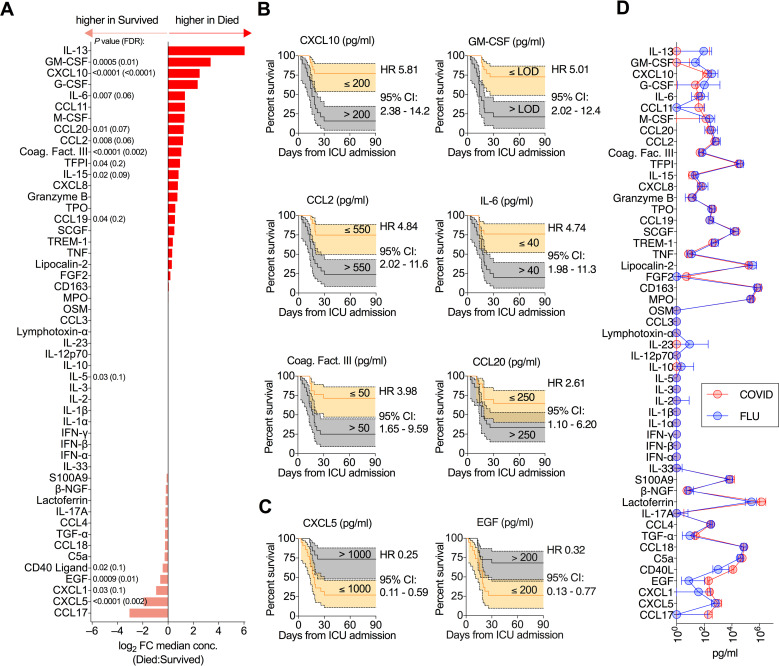
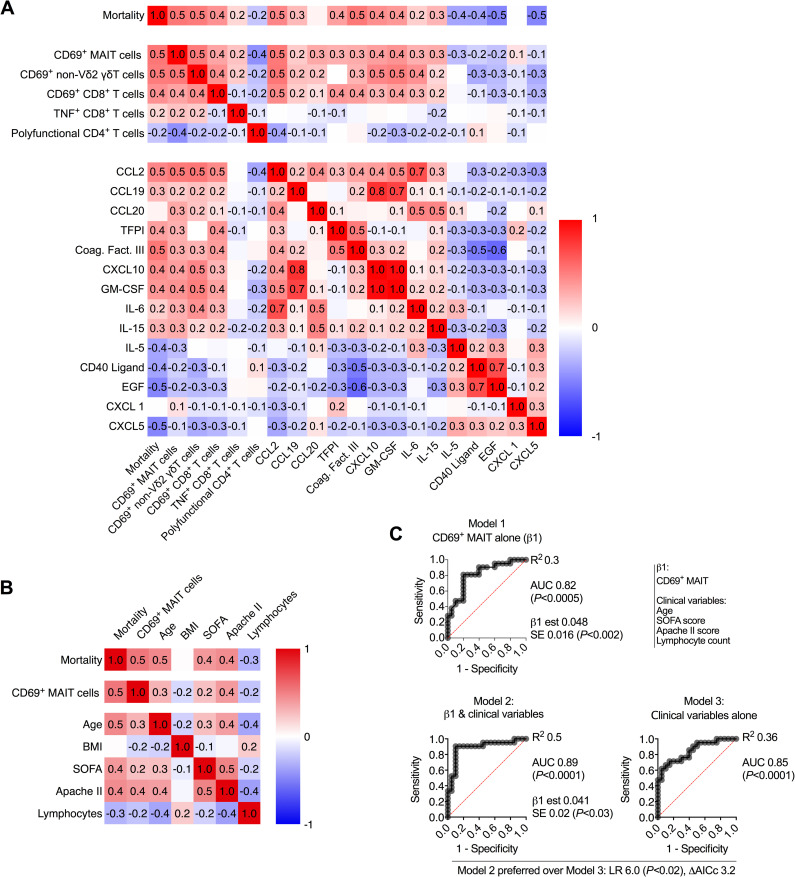
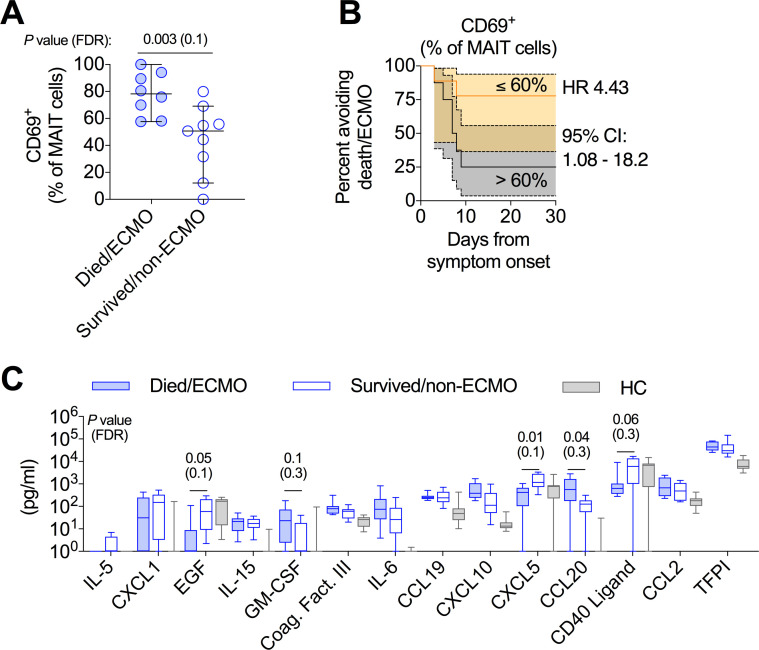
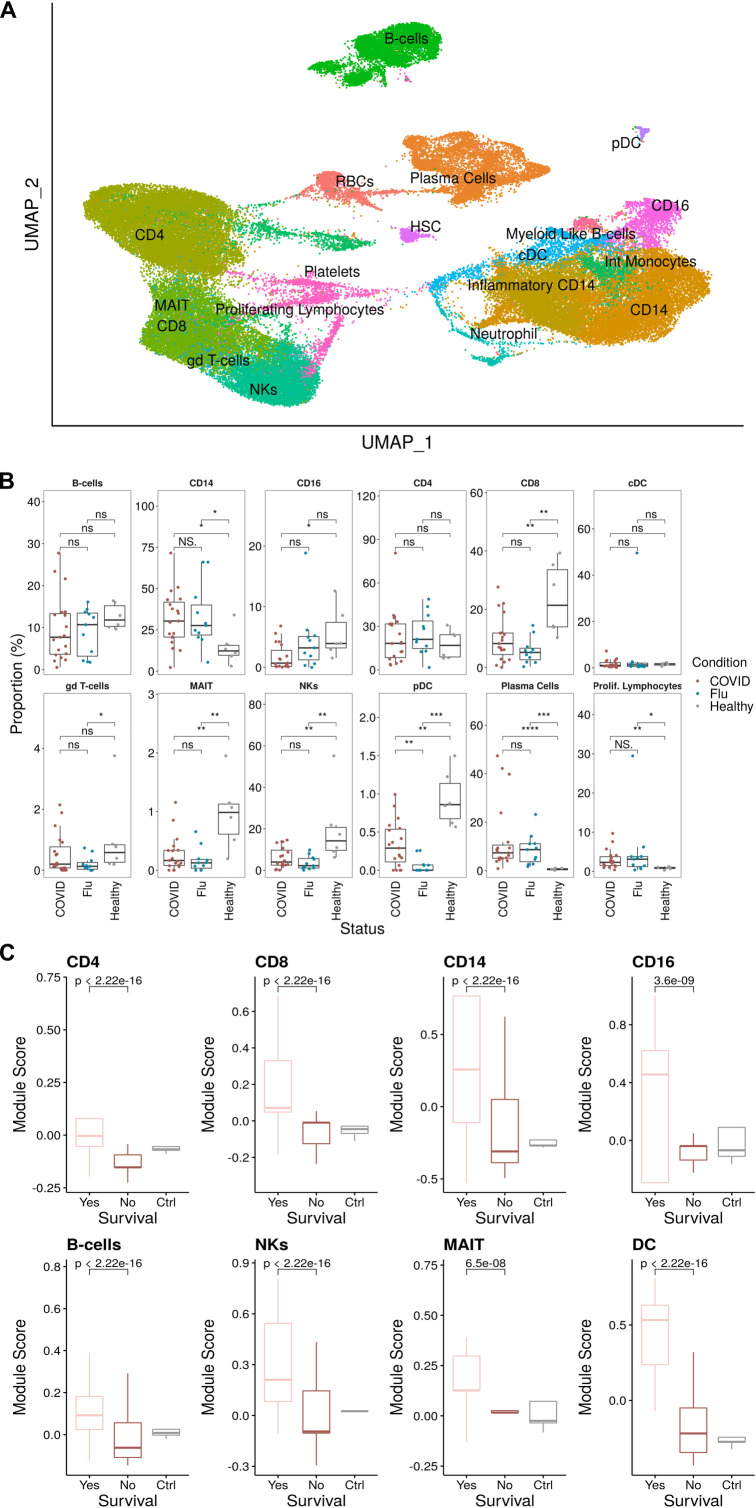
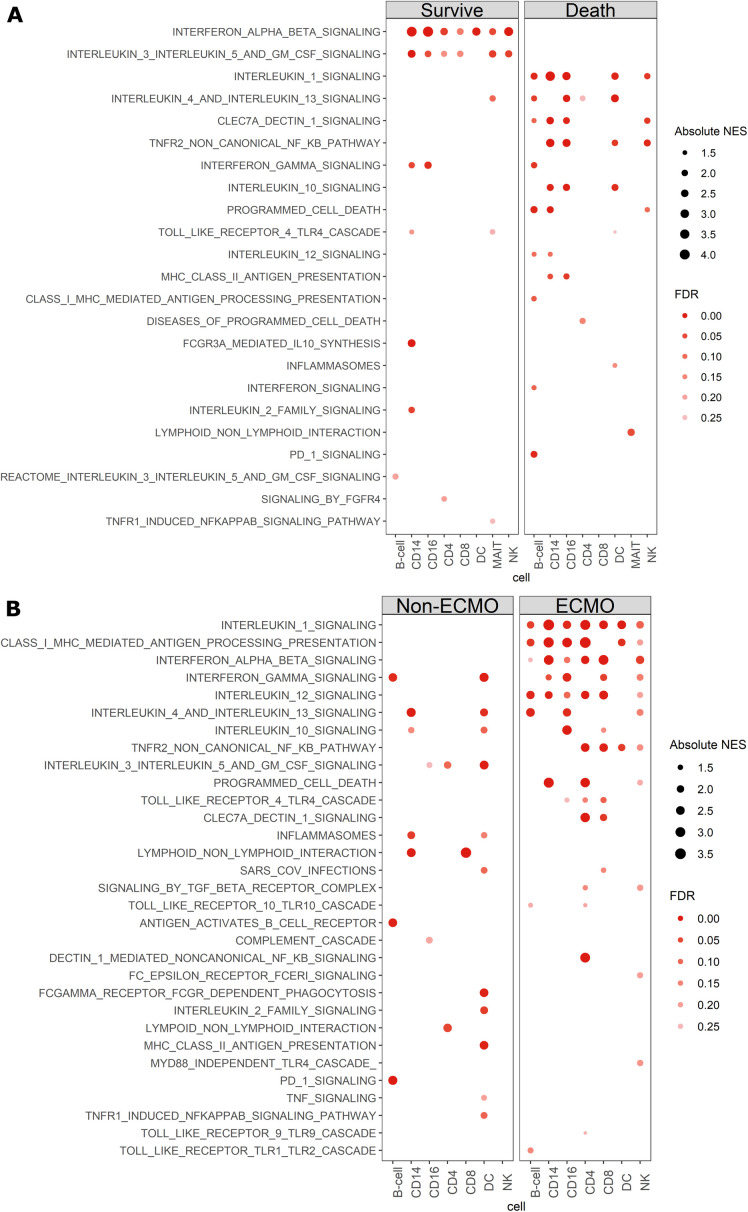
Prior studies have demonstrated that immunologic dysfunction underpins severe illness in COVID-19 patients, but have lacked an in-depth analysis of the immunologic drivers of death in the most critically ill patients. We performed immunophenotyping of viral antigen-specific and unconventional T cell responses, neutralizing antibodies, and serum proteins in critically ill patients with SARS-CoV-2 infection, using influenza infection, SARS-CoV-2-convalescent health care workers, and healthy adults as controls. We identify mucosal-associated invariant T (MAIT) cell activation as an independent and significant predictor of death in COVID-19 (HR = 5.92, 95% CI = 2.49-14.1). MAIT cell activation correlates with several other mortality-associated immunologic measures including broad activation of CD8+ T cells and non-Vδ2 γδT cells, and elevated levels of cytokines and chemokines, including GM-CSF, CXCL10, CCL2, and IL-6. MAIT cell activation is also a predictor of disease severity in influenza (ECMO/death HR = 4.43, 95% CI = 1.08-18.2). Single-cell RNA-sequencing reveals a shift from focused IFNα-driven signals in COVID-19 ICU patients who survive to broad pro-inflammatory responses in fatal COVID-19 -a feature not observed in severe influenza. We conclude that fatal COVID-19 infection is driven by uncoordinated inflammatory responses that drive a hierarchy of T cell activation, elements of which can serve as prognostic indicators and potential targets for immune intervention.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests:WH reports lecture fees from Gilead.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
