

Untangling the pathophysiologic link between coronary microvascular dysfunction and heart failure with preserved ejection fraction
- PMID: 34529791
- PMCID: PMC8599060
- DOI: 10.1093/eurheartj/ehab653
Untangling the pathophysiologic link between coronary microvascular dysfunction and heart failure with preserved ejection fraction
Abstract
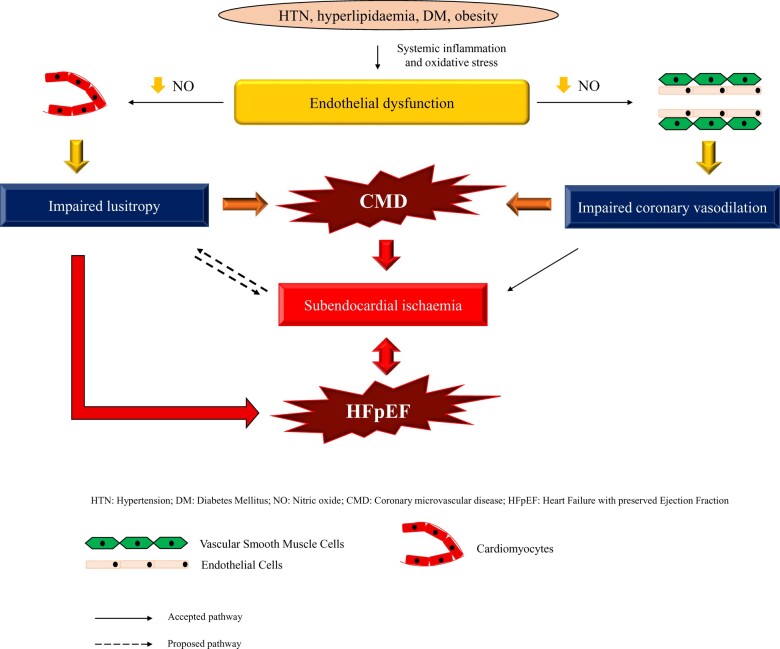
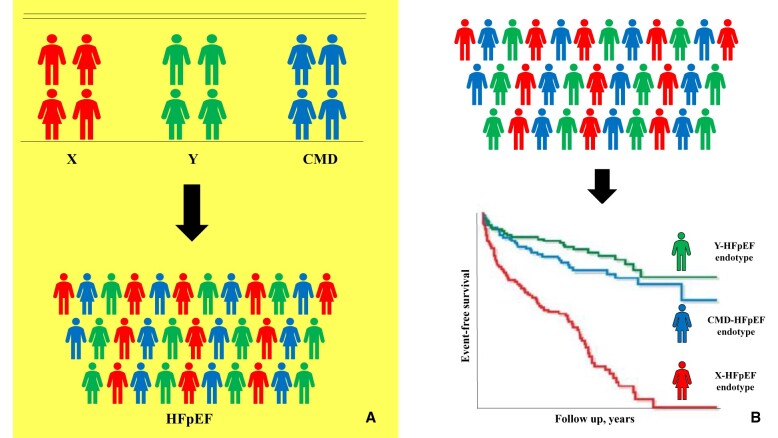
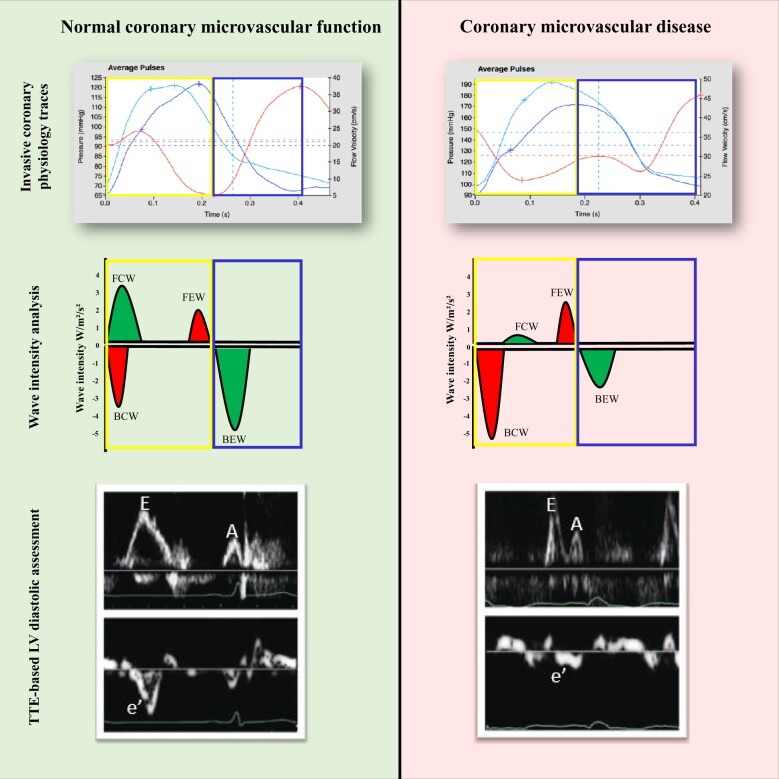
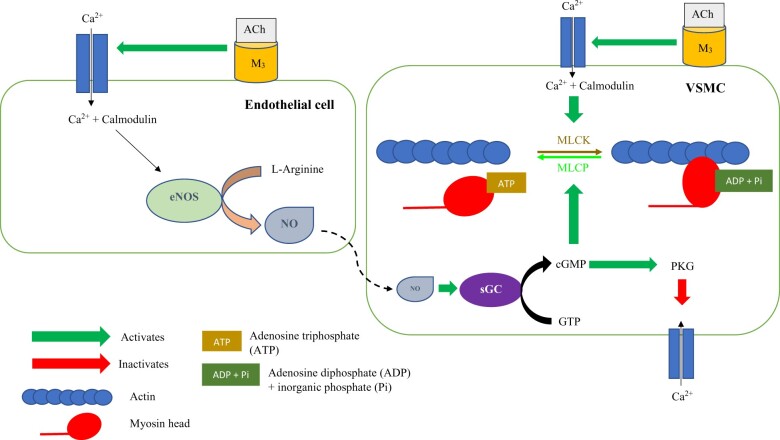
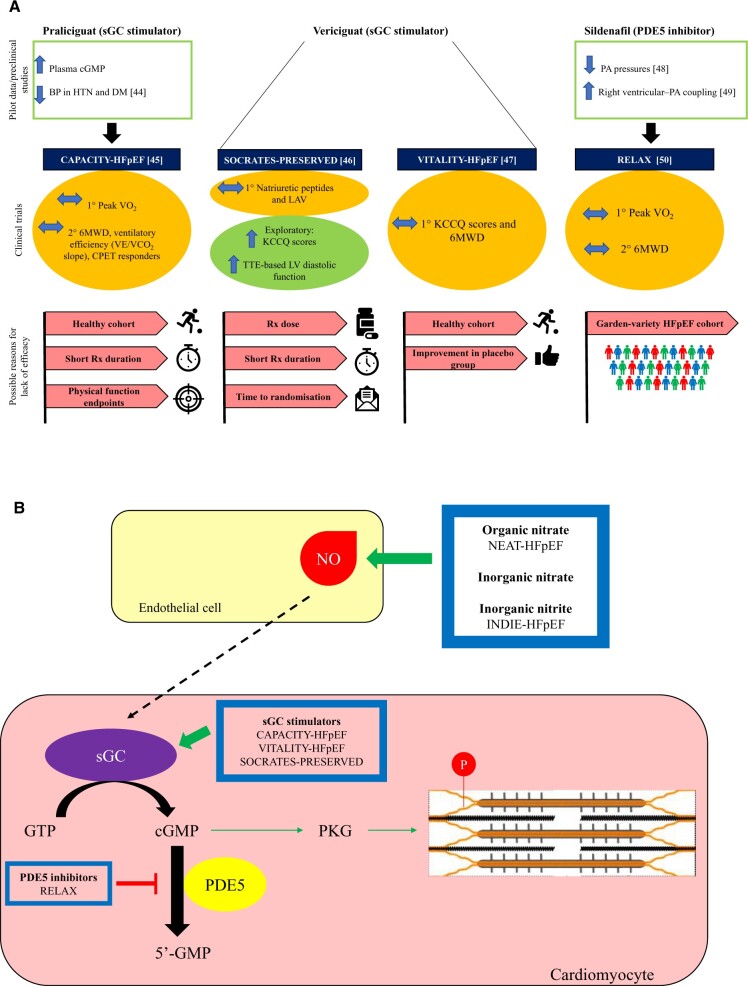
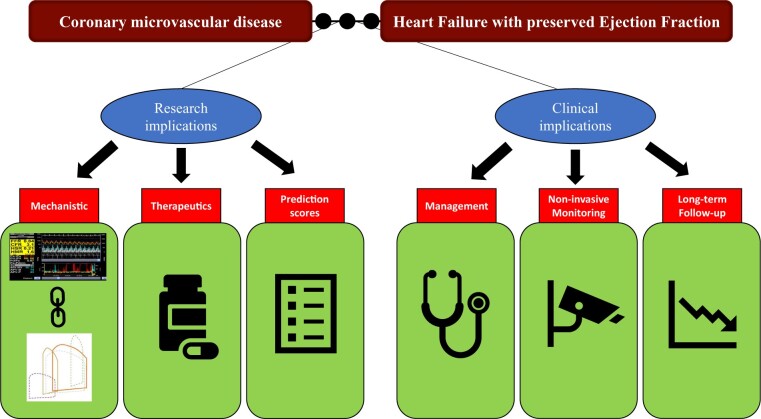
Coronary microvascular disease (CMD), characterized by impaired coronary flow reserve (CFR), is a common finding in patients with stable angina. Impaired CFR, in the absence of obstructive coronary artery disease, is also present in up to 75% of patients with heart failure with preserved ejection fraction (HFpEF). Heart failure with preserved ejection fraction is a heterogeneous syndrome comprising distinct endotypes and it has been hypothesized that CMD lies at the centre of the pathogenesis of one such entity: the CMD-HFpEF endotype. This article provides a contemporary review of the pathophysiology underlying CMD, with a focus on the mechanistic link between CMD and HFpEF. We discuss the central role played by subendocardial ischaemia and impaired lusitropy in the development of CMD-HFpEF, as well as the clinical and research implications of the CMD-HFpEF mechanistic link. Future prospective follow-up studies detailing outcomes in patients with CMD and HFpEF are much needed to enhance our understanding of the pathological processes driving these conditions, which may lead to the development of physiology-stratified therapy to improve the quality of life and prognosis in these patients.
Keywords: Coronary flow reserve; Coronary microvascular disease; Heart failure with preserved ejection fraction; Lusitropy; Subendocardial ischaemia.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Sara J, Widmer R, Matsuzawa Y, Lennon R, Lerman L, Lerman A. Prevalence of coronary microvascular dysfunction among patients with chest pain and nonobstructive coronary artery disease. JACC Cardiovasc Interv 2015;8:1445–1453. - PubMed
-
- Cannon R, Epstein S. “Microvascular angina” as a cause of chest pain with angiographically normal coronary arteries. Am J Cardiol 1988;61:1338–1343. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
