

Neuromyelitis optica spectrum disorders: from pathophysiology to therapeutic strategies
- PMID: 34530847
- PMCID: PMC8444436
- DOI: 10.1186/s12974-021-02249-1
Neuromyelitis optica spectrum disorders: from pathophysiology to therapeutic strategies
Abstract
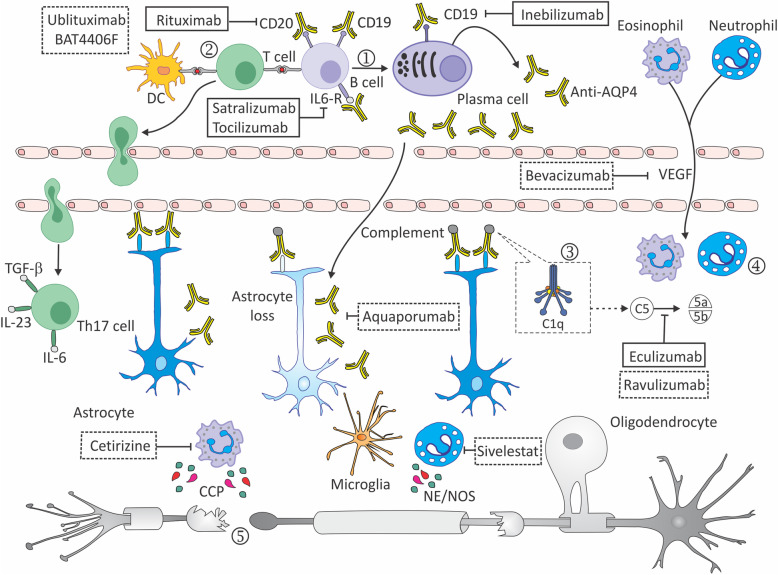
Neuromyelitis optica (NMO) is a chronic inflammatory autoimmune disease of the central nervous system (CNS) characterized by acute optic neuritis (ON) and transverse myelitis (TM). NMO is caused by a pathogenic serum IgG antibody against the water channel aquoporin 4 (AQP4) in the majority of patients. AQP4-antibody (AQP4-ab) presence is highly specific, and differentiates NMO from multiple sclerosis. It binds to AQP4 channels on astrocytes, triggering activation of the classical complement cascade, causing granulocyte, eosinophil, and lymphocyte infiltration, culminating in injury first to astrocyte, then oligodendrocytes followed by demyelination and neuronal loss. NMO spectrum disorder (NMOSD) has recently been defined and stratified based on AQP4-ab serology status. Most NMOSD patients experience severe relapses leading to permanent neurologic disability, making suppression of relapse frequency and severity, the primary objective in disease management. The most common treatments used for relapses are steroids and plasma exchange.Currently, long-term NMOSD relapse prevention includes off-label use of immunosuppressants, particularly rituximab. In the last 2 years however, three pivotal clinical trials have expanded the spectrum of drugs available for NMOSD patients. Phase III studies have shown significant relapse reduction compared to placebo in AQP4-ab-positive patients treated with satralizumab, an interleukin-6 receptor (IL-6R) inhibitor, inebilizumab, an antibody against CD19+ B cells; and eculizumab, an antibody blocking the C5 component of complement. In light of the new evidence on NMOSD pathophysiology and of preliminary results from ongoing trials with new drugs, we present this descriptive review, highlighting promising treatment modalities as well as auspicious preclinical and clinical studies.
Keywords: Aquaporin-4-antibody; Astrocyte; Complement; Neuroinflammation; Neuromyelitis optica spectrum disorders (NMOSD); Ongoing trials; Treatment.
© 2021. The Author(s).
Conflict of interest statement
Edgar Carnero Contentti has received reimbursement for developing educational presentations, educational and research grants, consultation fees, and/or travel stipends from Biogen, Bayer, Genzyme, Merck, Novartis, Roche, Raffo, and Teva. ECC has also received grants from LACTRIMS and Guthy-Jackson Charitable Foundation. Jorge Correale is a board member of Merck-Serono Argentina, Novartis Argentina, Genzyme LATAM, Genzyme global, Biogen-Idec LATAM and Merck-Serono LATAM. He is part of the Steering Committee for the clinical trials of Ofatumumab (Novartis Global). JC has received reimbursement for developing educational presentations for Merck-Serono Argentina, Merck-Serono LATAM, Biogen-Idec Argentina, Genzyme Argentina, Novartis Argentina, Novartis LATAM, Novartis Global and Roche Argentina, as well as professional travel/accommodation stipends.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
